

Viral co-detection of influenza virus and other respiratory viruses in hospitalized Brazilian patients during the first three years of the coronavirus disease (COVID)-19 pandemic: an epidemiological profile
- PMID: 39479210
- PMCID: PMC11521903
- DOI: 10.3389/fmicb.2024.1462802
Viral co-detection of influenza virus and other respiratory viruses in hospitalized Brazilian patients during the first three years of the coronavirus disease (COVID)-19 pandemic: an epidemiological profile
Abstract
Introduction: In Brazil, few studies were performed regarding the co-detection of respiratory viruses in hospitalized patients. In this way, the study aimed to describe the epidemiological profile of hospitalized patients due to influenza virus infection that presented co-detection with another respiratory virus.
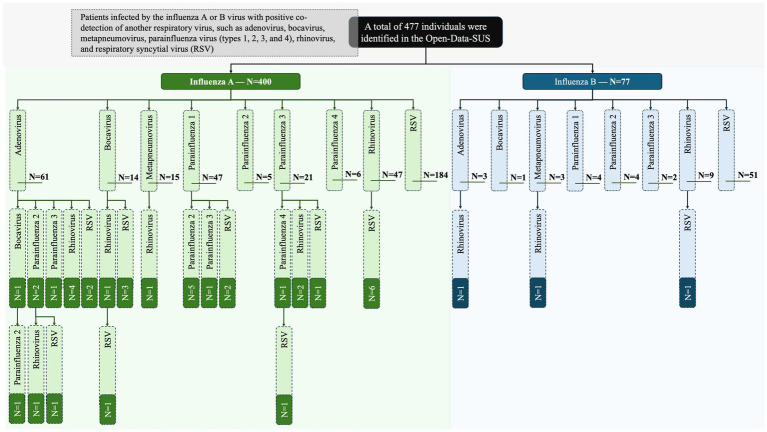
Methods: The epidemiological analysis was made by collecting data from Open-Data-SUS. The study comprised patients infected by the influenza A or B virus with positive co-detection of another respiratory virus, such as adenovirus, bocavirus, metapneumovirus, parainfluenza virus (types 1, 2, 3, and 4), rhinovirus, and respiratory syncytial virus (RSV). The markers [gender, age, clinical signs and symptoms, comorbidities, need for intensive care unit (ICU) treatment, and need for ventilatory support] were associated with the chance of death. The data was collected during the first three years of the coronavirus disease (COVID)-19 pandemic-from December 19, 2019, to April 06, 2023.
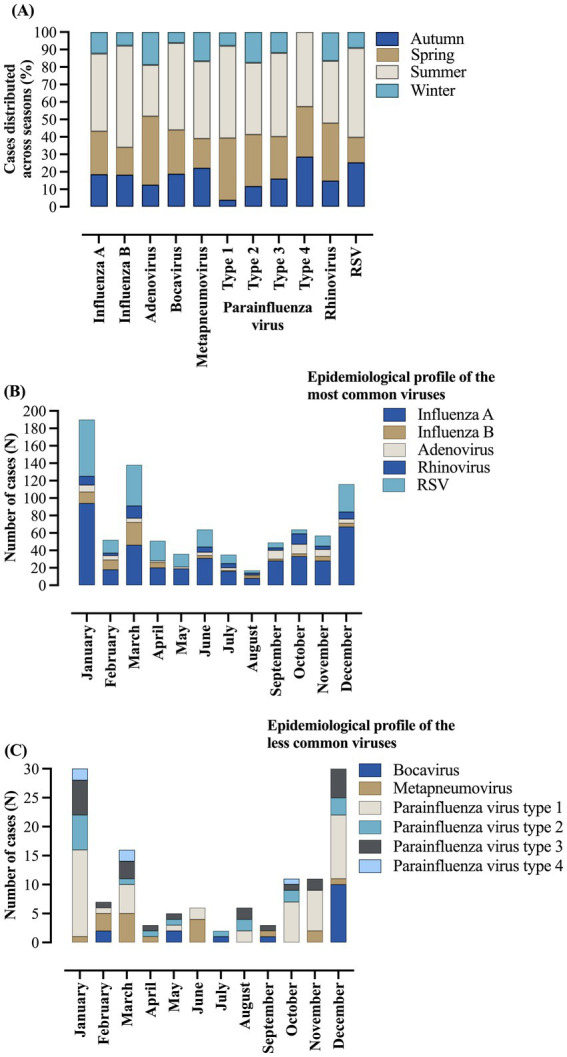
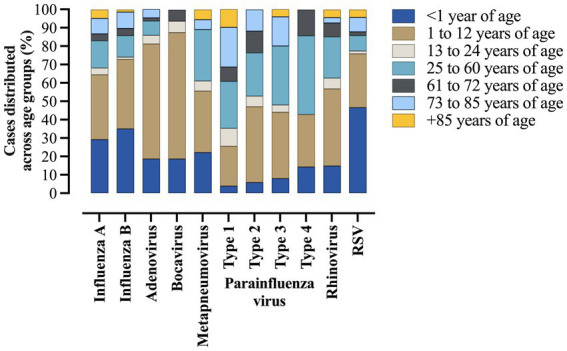
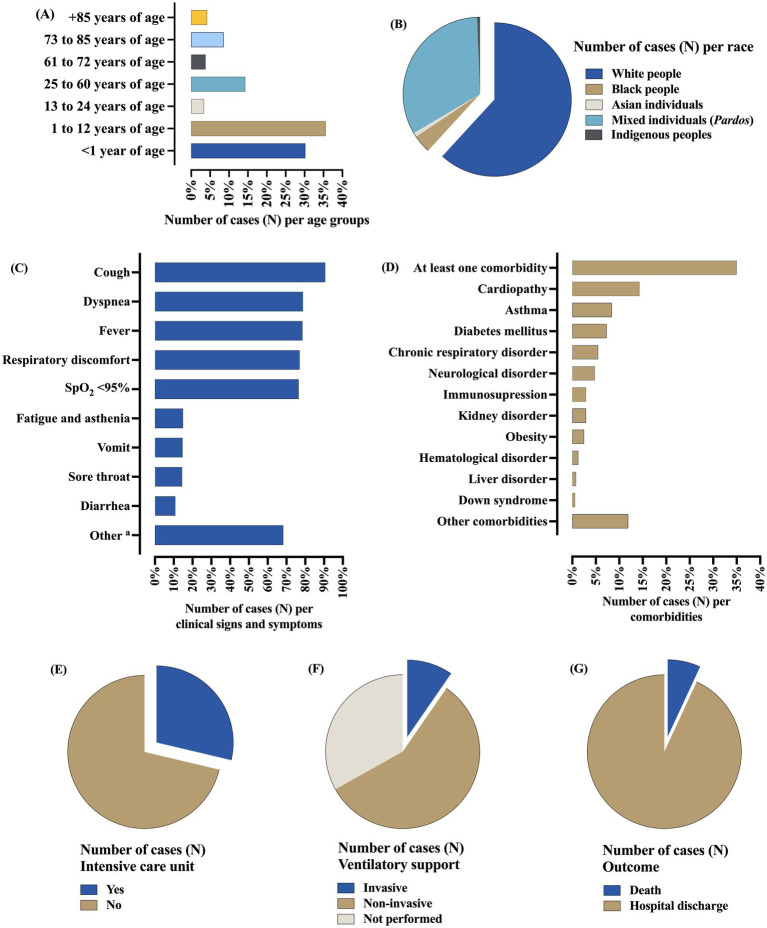
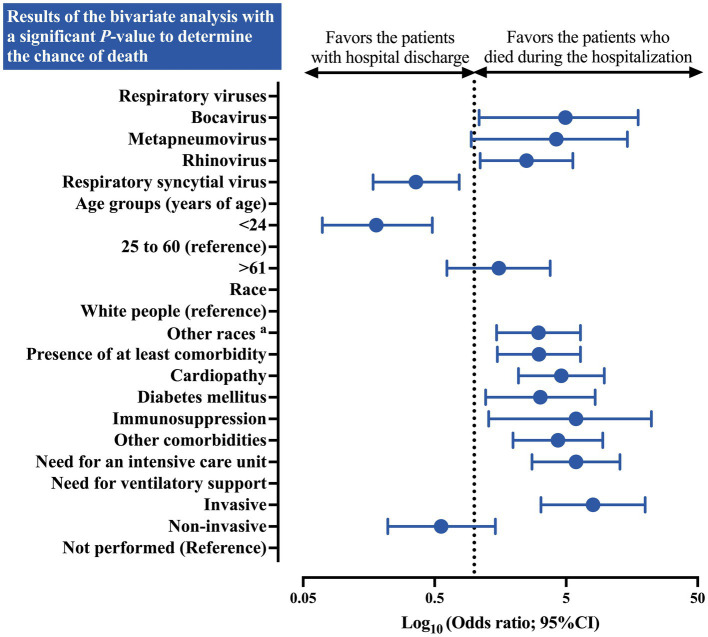
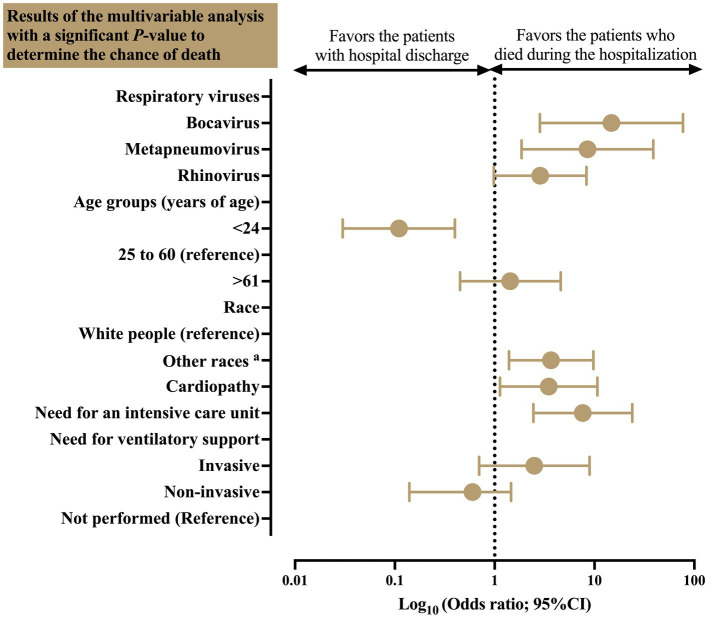
Results: A total of 477 patients were included, among them, the influenza A virus was detected in 400 (83.9%) cases. The co-detection occurred, respectively, for RSV (53.0%), rhinovirus (14.0%), adenovirus (13.4%), parainfluenza virus type 1 (10.7%), parainfluenza virus type 3 (5.2%), metapneumovirus (3.8%), parainfluenza virus type 2 (3.6%), bocavirus (3.4%), and parainfluenza virus type 4 (1.5%). The co-detection rate was higher in the male sex (50.7%), age between 0-12 years of age (65.8%), and white individuals (61.8%). The most common clinical symptoms were cough (90.6%), dyspnea (78.8%), and fever (78.6%). A total of 167 (35.0%) people had at least one comorbidity, mainly cardiopathy (14.3%), asthma (8.4%), and diabetes mellitus (7.3%). The need for ICU treatment occurred in 147 (30.8%) cases, with most of them needing ventilatory support (66.8%), mainly non-invasive ones (57.2%). A total of 33 (6.9%) patients died and the main predictors of death were bocavirus infection (OR = 14.78 [95%CI = 2.84-76.98]), metapneumovirus infection (OR = 8.50 [95%CI = 1.86-38.78]), race (other races vs. white people) (OR = 3.67 [95%CI = 1.39-9.74]), cardiopathy (OR = 3.48 [95%CI = 1.13-10.71]), and need for ICU treatment (OR = 7.64 [95%CI = 2.44-23.92]).
Conclusion: Co-detection between the influenza virus and other respiratory viruses occurred, mainly with RSV, rhinovirus, and adenovirus being more common in men, white people, and in the juvenile phase. Co-detection of influenza virus with bocavirus and metapneumovirus was associated with an increased chance of death. Other factors such as race, cardiopathy, and the need for an ICU were also associated with a higher chance of death.
Keywords: adenovirus; bocavirus; influenza virus; metapneumovirus; parainfluenza virus; respiratory syncytial virus; rhinovirus; severe acute respiratory syndrome coronavirus 2.
Copyright © 2024 Siqueira, Bredariol, Boschiero and Marson.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Adlhoch C., Sneiderman M., Martinuka O., Melidou A., Bundle N., Fielding J., et al. . (2021). Spotlight influenza: the 2019/20 influenza season and the impact of COVID-19 on influenza surveillance in the WHO European region. Euro Surveill. 26:2100077. doi: 10.2807/1560-7917.ES.2021.26.40.2100077, PMID: - DOI - PMC - PubMed
-
- Ambrosioni J., Bridevaux P.-O., Wagner G., Mamin A., Kaiser L. (2014). Epidemiology of viral respiratory infections in a tertiary care Centre in the era of molecular diagnosis, Geneva, Switzerland, 2011–2012. Clin. Microbiol. Infect. 20, O578–O584. doi: 10.1111/1469-0691.12525, PMID: - DOI - PMC - PubMed
-
- Ambrożej D., Orzołek I., Makrinioti H., Castro-Rodriguez J. A., Camargo C. A., Hasegawa K., et al. . (2024). Association of respiratory virus types with clinical features in bronchiolitis: implications for virus testing strategies. A systematic review and meta-analysis. Paediatr. Respir. Rev. 49, 34–42. doi: 10.1016/j.prrv.2023.09.003, PMID: - DOI - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous