

Anthracycline Cardiotoxicity in Adult Cancer Patients: JACC: CardioOncology State-of-the-Art Review
- PMID: 39479333
- PMCID: PMC11520218
- DOI: 10.1016/j.jaccao.2024.07.016
Anthracycline Cardiotoxicity in Adult Cancer Patients: JACC: CardioOncology State-of-the-Art Review
Abstract
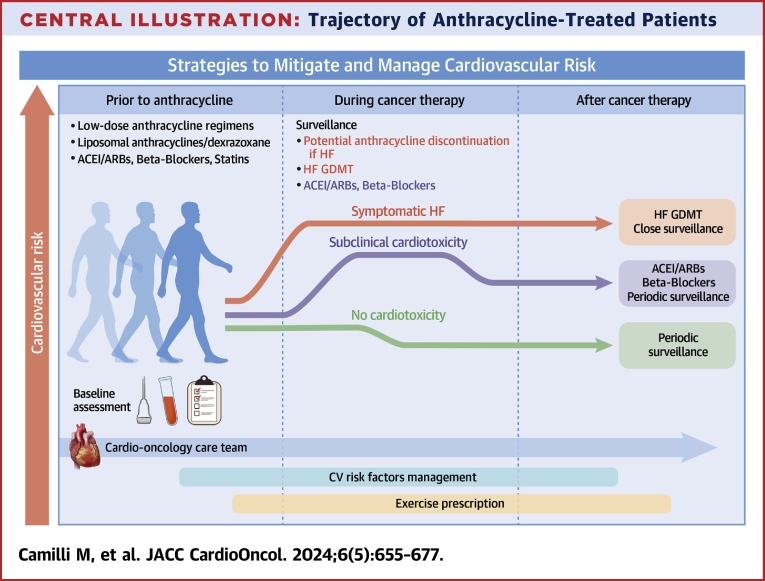
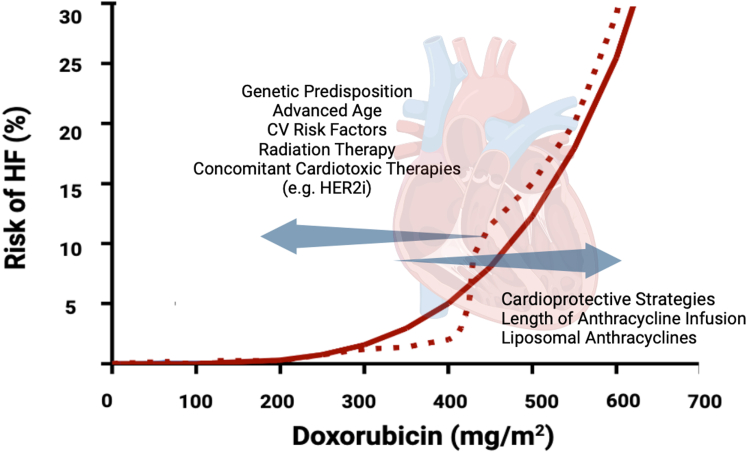
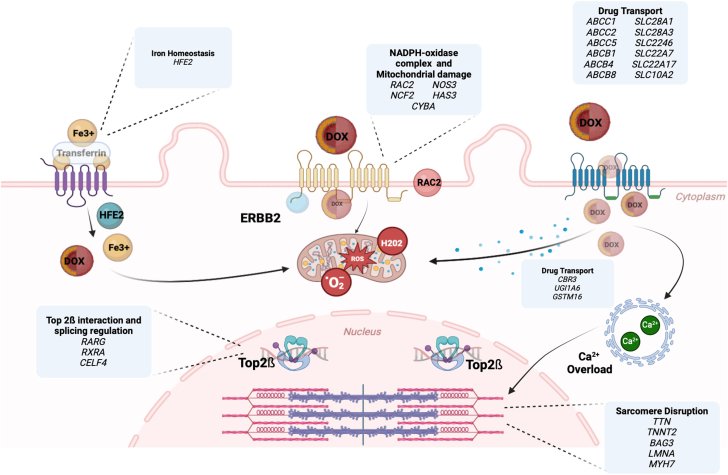
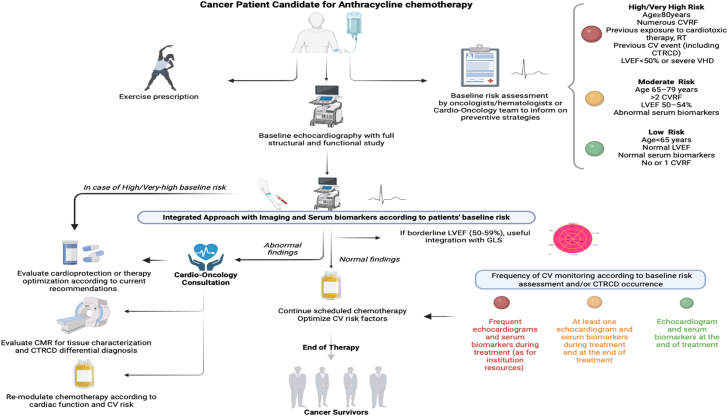
Since their introduction in the 1960s, anthracyclines have been a significant breakthrough in oncology, introducing dramatic changes in the treatment of solid and hematologic malignancies. Although new-generation targeted drugs and cellular therapies are revolutionizing contemporary oncology, anthracyclines remain the cornerstone of treatment for lymphomas, acute leukemias, and soft tissue sarcomas. However, their clinical application is limited by a dose-dependent cardiotoxicity that can reduce cardiac performance and eventually lead to overt heart failure. The field of cardio-oncology has emerged to safeguard the cardiovascular health of cancer patients receiving these therapies. It focuses on controlling risk factors, implementing preventive strategies, ensuring appropriate surveillance, and managing complications. This state-of-the-art review summarizes the current indications for anthracyclines in modern oncology, explores recent evidence on pathophysiology and epidemiology, and discusses advances in cardioprotection measures in the anthracycline-treated patient. Additionally, it highlights key clinical challenges and research gaps in this area.
Keywords: anthracycline; biomarkers; cancer survivorship; diagnosis; heart failure.
© 2024 The Authors.
Conflict of interest statement
The authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures



References
-
- Minotti G., Menna P., Salvatorelli E., Cairo G., Gianni L. Anthracyclines: molecular advances and pharmacologic developments in antitumor activity and cardiotoxicity. Pharmacol Rev. 2004;56(2):185–229. - PubMed
-
- Levis B.E., Binkley P.F., Shapiro C.L. Cardiotoxic effects of anthracycline-based therapy: what is the evidence and what are the potential harms? Lancet Oncol. 2017;18(8):e445–e456. - PubMed
-
- World Health Organization . World Health Organization; 2023. World Health Organization Model List of Essential Medicines-23rd List, 2023.
Publication types
LinkOut - more resources
Full Text Sources
Medical
