

A Randomized Trial of Drug Route in Out-of-Hospital Cardiac Arrest
- PMID: 39480216
- PMCID: PMC7616768
- DOI: 10.1056/NEJMoa2407780
A Randomized Trial of Drug Route in Out-of-Hospital Cardiac Arrest
Abstract
Background: In patients with out-of-hospital cardiac arrest, the effectiveness of drugs such as epinephrine is highly time-dependent. An intraosseous route of drug administration may enable more rapid drug administration than an intravenous route; however, its effect on clinical outcomes is uncertain.
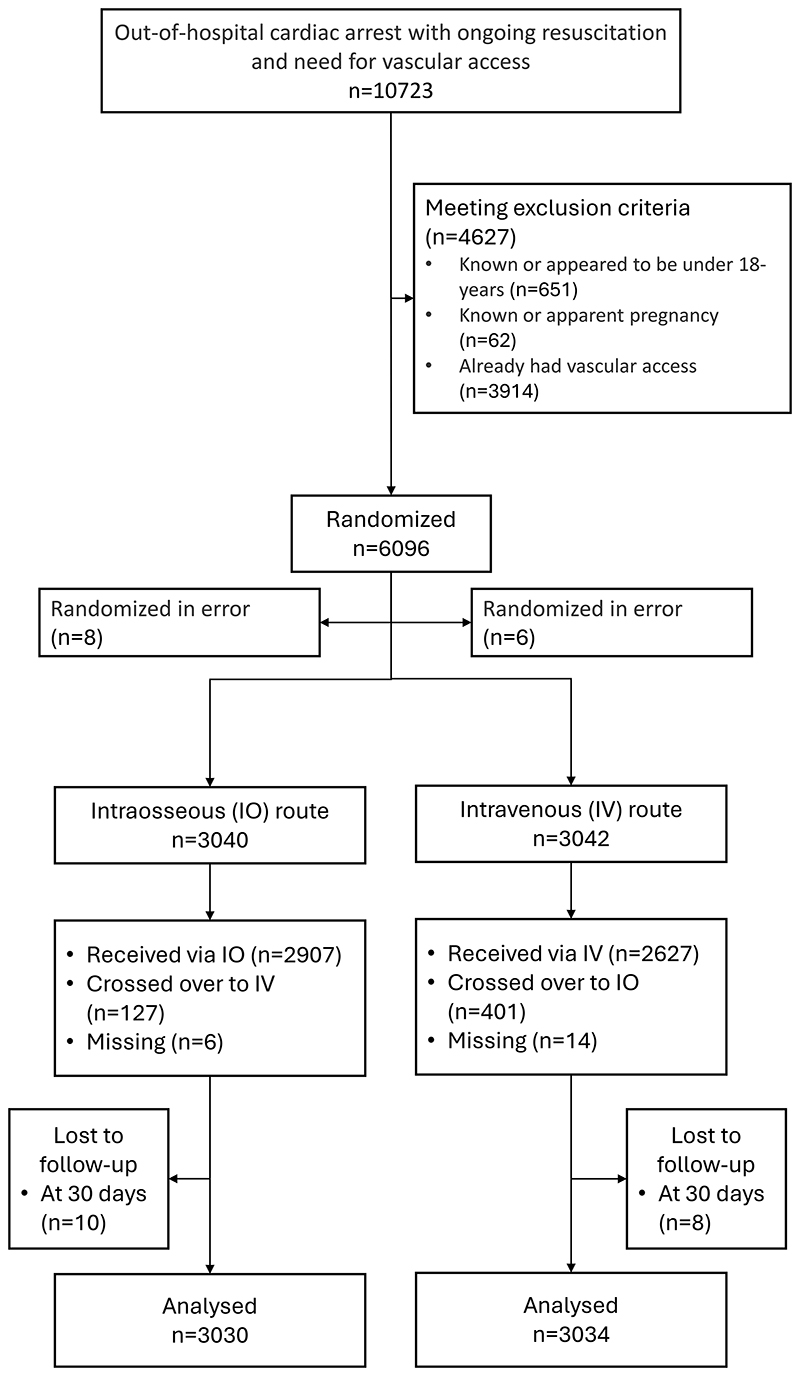
Methods: We conducted a multicenter, open-label, randomized trial across 11 emergency medical systems in the United Kingdom that involved adults in cardiac arrest for whom vascular access for drug administration was needed. Patients were randomly assigned to receive treatment from paramedics by means of an intraosseous-first or intravenous-first vascular access strategy. The primary outcome was survival at 30 days. Key secondary outcomes included any return of spontaneous circulation and favorable neurologic function at hospital discharge (defined by a score of 3 or less on the modified Rankin scale, on which scores range from 0 to 6, with higher scores indicating greater disability). No adjustment for multiplicity was made.
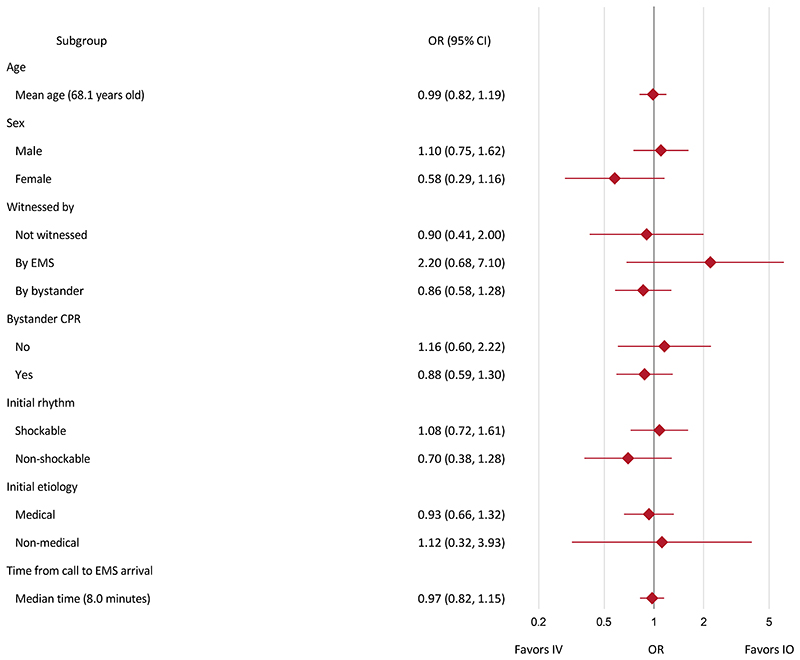
Results: A total of 6082 patients were assigned to a trial group: 3040 to the intraosseous group and 3042 to the intravenous group. At 30 days, 137 of 3030 patients (4.5%) in the intraosseous group and 155 of 3034 (5.1%) in the intravenous group were alive (adjusted odds ratio, 0.94; 95% confidence interval [CI], 0.68 to 1.32; P = 0.74). At the time of hospital discharge, a favorable neurologic outcome was observed in 80 of 2994 patients (2.7%) in the intraosseous group and in 85 of 2986 (2.8%) in the intravenous group (adjusted odds ratio, 0.91; 95% CI, 0.57 to 1.47); a return of spontaneous circulation at any time occurred in 1092 of 3031 patients (36.0%) and in 1186 of 3035 patients (39.1%), respectively (adjusted odds ratio, 0.86; 95% CI, 0.76 to 0.97). During the trial, one adverse event, which occurred in the intraosseous group, was reported.
Conclusions: Among adults with out-of-hospital cardiac arrest requiring drug therapy, the use of an intraosseous-first vascular access strategy did not result in higher 30-day survival than an intravenous-first strategy. (Funded by the National Institute for Health and Care Research; PARAMEDIC-3 ISRCTN Registry number, ISRCTN14223494.).
Copyright © 2024 Massachusetts Medical Society.
Figures
Comment in
-
Initial Intraosseous or Intravenous Access for Out-of-Hospital Cardiac Arrest.N Engl J Med. 2025 May 1;392(17):1763. doi: 10.1056/NEJMc2502751. N Engl J Med. 2025. PMID: 40305723 No abstract available.
-
Initial Intraosseous or Intravenous Access for Out-of-Hospital Cardiac Arrest.N Engl J Med. 2025 May 1;392(17):1763. doi: 10.1056/NEJMc2502751. N Engl J Med. 2025. PMID: 40305724 No abstract available.
-
Initial Intraosseous or Intravenous Access for Out-of-Hospital Cardiac Arrest. Reply.N Engl J Med. 2025 May 1;392(17):1763-1764. doi: 10.1056/NEJMc2502751. N Engl J Med. 2025. PMID: 40305725 No abstract available.
-
Initial Intraosseous or Intravenous Access for Out-of-Hospital Cardiac Arrest. Reply.N Engl J Med. 2025 May 1;392(17):1764. doi: 10.1056/NEJMc2502751. N Engl J Med. 2025. PMID: 40305726 No abstract available.
References
-
- Perkins GD, Ji C, Deakin CD, et al. A Randomized Trial of Epinephrine in Out-of-Hospital Cardiac Arrest. New England Journal of Medicine. 2018;379(8):711–721. - PubMed
-
- Kudenchuk PJ, Brown SP, Daya M, et al. Amiodarone, Lidocaine, or Placebo in Out-of-Hospital Cardiac Arrest. New England Journal of Medicine. 2016;374(18):1711–1722. - PubMed
-
- Rahimi M, Dorian P, Cheskes S, Lebovic G, Lin S. Effect of Time to Treatment With Antiarrhythmic Drugs on Return of Spontaneous Circulation in Shock-Refractory Out-of-Hospital Cardiac Arrest. Journal of the American Heart Association. 2022;11(6):e023958. doi: 10.1161/JAHA.121.023958. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources