

Global outcomes and prognosis for relapsed/refractory mature T-cell and NK-cell lymphomas: results from the PETAL consortium
- PMID: 39481087
- PMCID: PMC11821408
- DOI: 10.1182/bloodadvances.2024014674
Global outcomes and prognosis for relapsed/refractory mature T-cell and NK-cell lymphomas: results from the PETAL consortium
Abstract
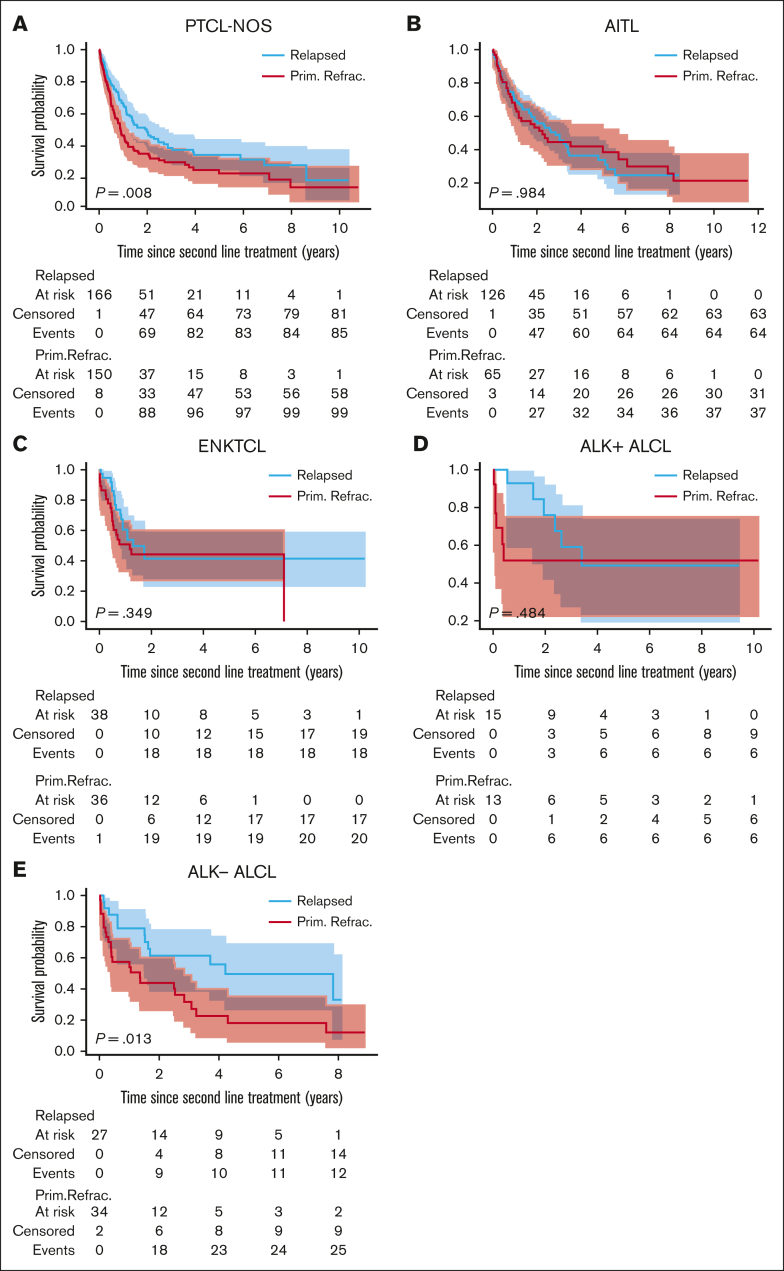
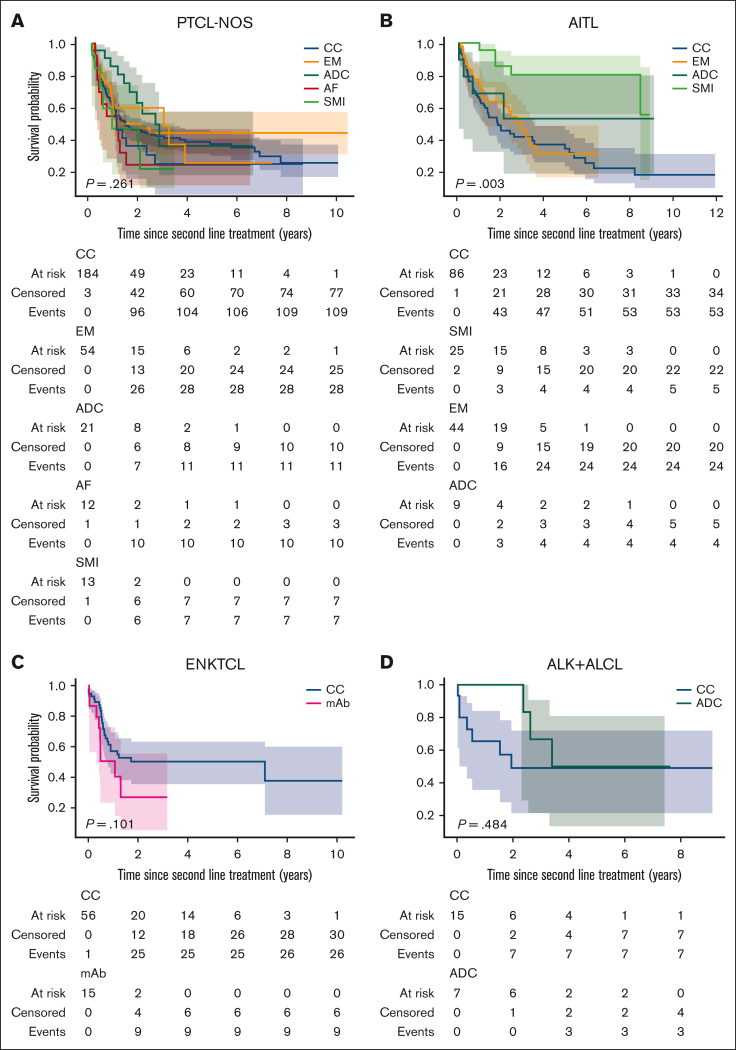
Variances in global access to drugs and treatment practices make it challenging to understand the benefit of contemporary therapies in patients with relapsed and refractory (R/R) mature T-cell and natural killer-cell lymphomas (MTCL and MNKCL). We conducted an international retrospective cohort study of 925 patients with R/R MTCL and MNKCL. In peripheral T-cell lymphoma-not otherwise specified and anaplastic lymphoma kinase-negative anaplastic large cell lymphoma (ALK- ALCL), patients with relapsed lymphoma demonstrated a superior median overall survival (OS) relative to refractory from the time of second-line treatment. We identified several independent predictors of OS for R/R lymphoma including age >60 years, primary refractory disease, histological subtype other than angioimmunoblastic T-cell lymphoma (AITL), extranodal sites >1, Ki67 ≥40%, and absolute lymphocyte count less than the lower limit of normal. A multivariable model incorporating these formed the basis for a prognostic index for R/R TCL, in which patients are stratified into low-risk (0-1 risk factor), intermediate-risk (2-3 risk factors), or high-risk (≥4 risk factors) groups, which were associated with 3-year OS of 57.14%, 23.3%, and 7%, respectively. Patients received either a "novel" single agent (SA; 35%) or cytotoxic chemotherapy (CC; 60%) for their second-line treatment. Higher progression-free survival was observed with SA over CC for the entire cohort with a higher 3-year OS in AITL and ALK- ALCL. Among the SA, small-molecule inhibitors demonstrated OS advantage relative to CC in AITL. Our results highlight continued efficacy of novel drugs globally and the potential of a new prediction model in informing heterogeneous prognosis within the R/R population of MTCL and MNKCL.
© 2024 by The American Society of Hematology. Licensed under Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International (CC BY-NC-ND 4.0), permitting only noncommercial, nonderivative use with attribution. All other rights reserved.
Conflict of interest statement
Conflict-of-interest disclosure: C.C. treports honoraria and consultancy fees from Roche, AbbVie, Janssen, AstraZeneca (AZ), Eli Lilly and Company (Lylli), and Takeda. S.M.H. reports consultancy fees from ONO Pharmaceuticals, Tubulis, Abcuro Inc, Cimieo Therapeutics, Auxilius Pharma, Secura Bio, Shoreline Biosciences, Inc, and Yingli Pharma Limited; research funding from Affimed, Celgene, ADC Therapeutics, Millenium, CRISPR Therapeutics, Seattle Genetics, and Verastem/Secura Bio; and consultancy fees and research funding from Daiichi Sankyo, Trillium Therapeutics, Kyowa Hakko Kirin, and Takeda. E.J. reports research funding from Celgene, Pharmacyclics, and Hoffmann-LaRoche; honoraria and research funding from Merck; honoraria from Daiichi, Bristol Myers Squibb (BMS), and Bayer; and patents and royalties with UpToDate. H.J. reports research funding from ImmunoACT, Zydus Pharmaceuticals, and Intas Pharmaceuticals. C.V.D.W. reports ending employment in the past 24 months and membership on an entity's board of directors or advisory committees of Cartherics Pty Ltd. H.M.P. reports speakers bureau fees from Takeda, Merck, Mallinkrodt, and Mundipharma. F.F. reports honoraria from Secura Bio, Daiichi Sankyo, Kyowa, Conjupro, and Astex; and speakers bureau fees from Seagen and Acrotech. B.C. reports membership on an entity's board of directors or advisory committees in Kite-Gilead, AbbVie, Janssen, Celgene-BMS, BeiGene, and Takeda; and speakers bureau fees from Kite-Gilead, AbbVie, Janssen, Novartis, Lilly, and Roche. P.L.Z. reports membership on an entity's board of directors or advisory committees in Servier, Celltrion, Sandoz, Gilead, Secura Bio, Janssen-Cilag, BMS, Novartis, Antibody-drug conjugate (ADC) Therapeutics, Incyte, AstraZeneca, Merck Sharp & Dohme (MSD), EUSA Pharma, Takeda, Roche, Kyowa Kirin, and BeiGene; speakers bureau fees from Servier, Celltrion, Gilead, Janssen-Cilag, BMS, Novartis, Incyte, AstraZeneca, MSD, Takeda, Roche, EUSA Pharma, Kyowa Kirin, and BeiGene; and consultancy fees from Novartis, MSD, and EUSA Pharma. W.-S.K. reports research funding from Sanofi, BeiGene, Boryong, Roche, Kyowa Kirin, and Donga. E.V. reports research funding from MSD. C.S. reports current employment with Biogen Digital Health. E. Marchi reports research funding from Merck, Celgene/BMS, Astex Pharmaceutical/Myeloid Pharmaceuticals, and Dren Bio; membership on an entity's board of directors or advisory committees in Dren Bio; and other interests including data safety monitoring committee fees from Everest Clinical Research. S.J. reports consultancy fees from Mersana Therapeutics, Myeloid Therapeutics, SIRPant Immunotherapeutics, and Abcuro Inc; membership on an entity's board of directors or advisory committees in Mersana Therapeutics, Myeloid Therapeutics, SIRPant Immunotherapeutics, Abcuro Inc, Secura Bio, Daiichi Sankyo, and CRISPR Therapeutics; and research funding from Daiichi Sankyo, SIRPant Immunotherapeutics, Acrotech Limited Liability Company (LLC), and Abcuro Inc. The remaining authors declare no competing financial interests.
Figures








References
-
- Lansigan F, Horwitz SM, Pinter-Brown LC, et al. Outcomes for relapsed and refractory peripheral T-cell lymphoma patients after front-line therapy from the COMPLETE registry. Acta Haematol. 2020;143(1):40–50. - PubMed
-
- Ma H, Cheng B, Falchi L, et al. Survival benefit in patients with peripheral T-cell lymphomas after treatments with novel therapies and clinical trials. Hematol Oncol. 2020;38(1):51–58. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
