

Effects of Dietary Approaches and Exercise Interventions on Gestational Diabetes Mellitus: A Systematic Review and Bayesian Network Meta-analysis
- PMID: 39481539
- PMCID: PMC11629230
- DOI: 10.1016/j.advnut.2024.100330
Effects of Dietary Approaches and Exercise Interventions on Gestational Diabetes Mellitus: A Systematic Review and Bayesian Network Meta-analysis
Abstract
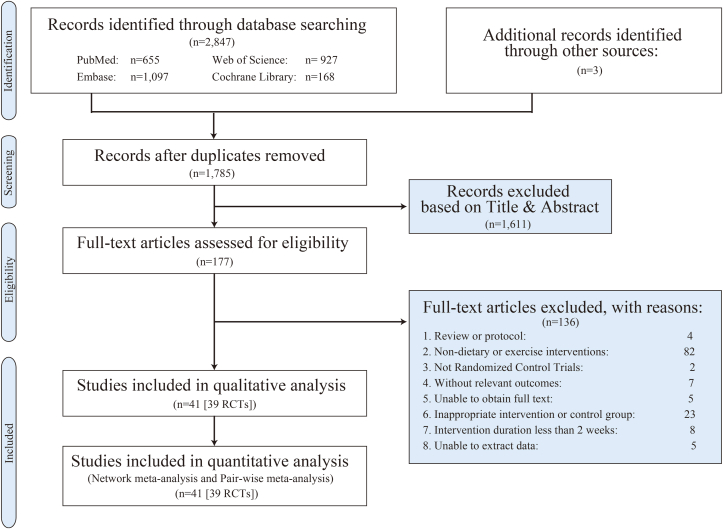
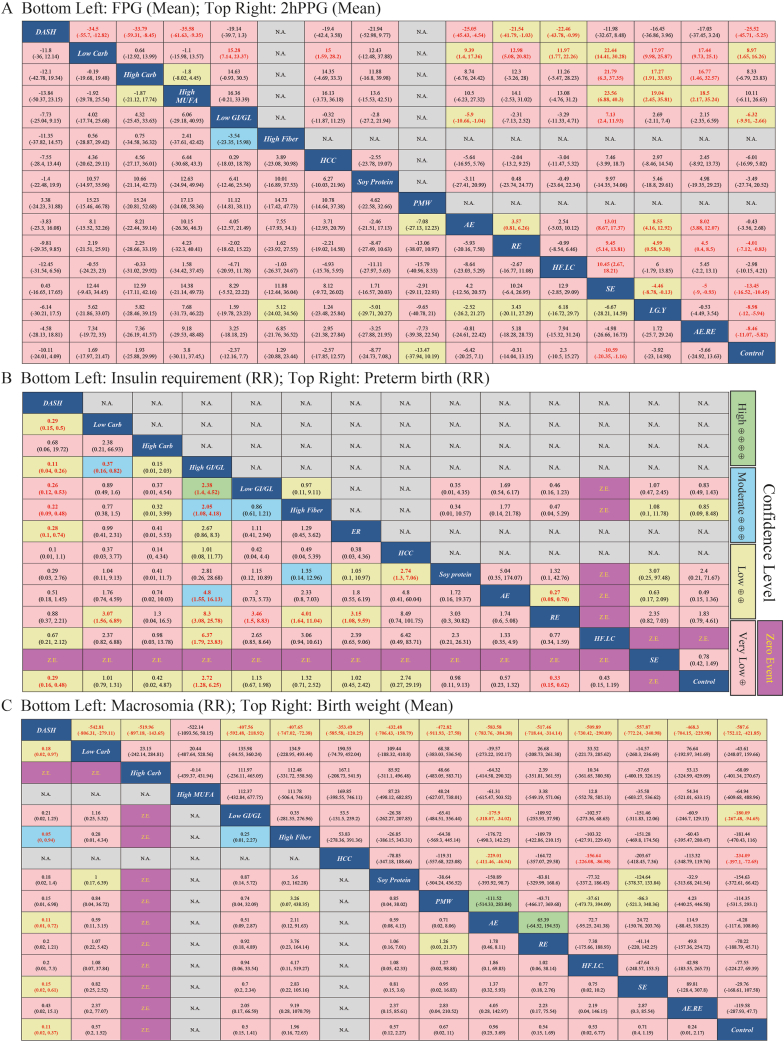
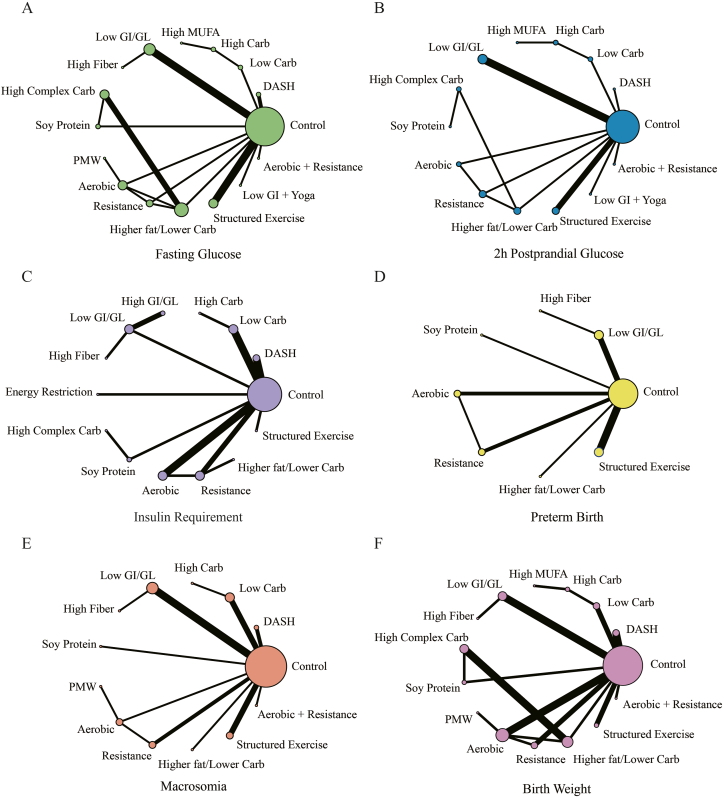
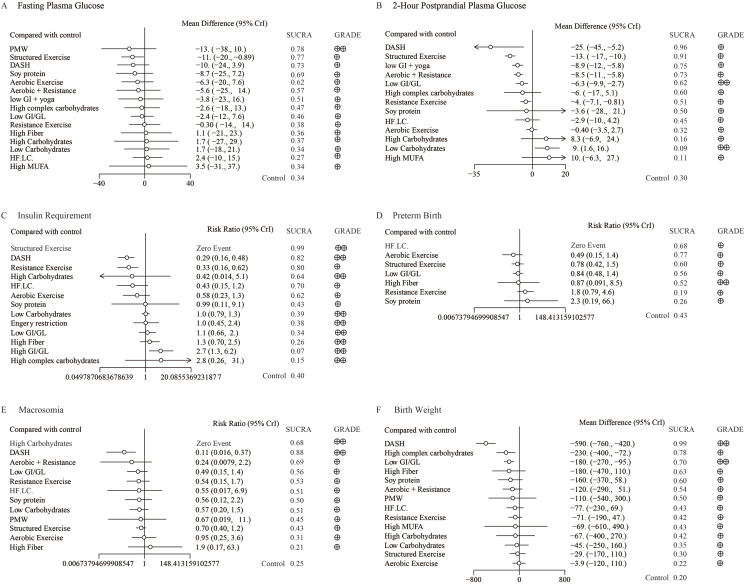
Although lifestyle interventions are recommended as the frontline therapeutic strategy for women with gestational diabetes mellitus (GDM), the optimal dietary regimen or form of exercise has yet to be definitively established. We aimed to compare the effectiveness of lifestyle therapies for GDM. Four databases (PubMed, Web of Science, EMBASE, and Cochrane Library) were systematically searched by multiple researchers for randomized controlled trials (RCTs). RCTs comparing lifestyle therapies to treat GDM with control or another treatment were included. Data extraction and synthesis were performed, estimating mean differences (MDs) or relative risk (RR) through pair-wise and network meta-analysis with a randomized or fixed-effects model when appropriate. The primary outcomes were maternal glucose control, birth weight of newborns, macrosomia and preterm birth rate, and rate of need for insulin therapy. In total, 39 trials with information obtained from 2712 women assessed 15 treatments. After sensitivity analysis, we confirmed the dietary approaches to stop hypertension (DASH) diet [MD: -11.52; 95% credible intervals (CrIs): -14.01, -9.07, very low certainty of evidence (CoE)] and low glycemic index (GI) diets (MD: -6.3; 95% CrI: -9.9, -2.7, low CoE) have shown significant advantages in fasting plasma glucose and 2-h postprandial glucose control, respectively. Furthermore, the DASH diet and resistance exercise reduced insulin requirements independently by 71% (95% CrI: 52%, 84%) and 67% (95% CrI: 48%, 85%), respectively. Additionally, both the DASH (MD: -587.6; 95% CrI: -752.12, -421.85, low CoE) and low GI diets (MD: -180.09, 95% CrI: -267.48, -94.65, low CoE) reduced birth weight significantly, with the DASH diet also demonstrating effects in reducing macrosomia by 89% (95% CrI: 53%, 98%) and lowering the cesarean section rate by 46% (95% CI: 27%, 60%). However, exercise did not affect infant outcomes. Our findings suggest that the DASH diet and low GI diet and resistance exercise may be beneficial for maternal outcomes in pregnancies with GDM. The impact on infants is primarily observed through dietary interventions. Future research, characterized by higher quality and evidence grades, is necessary to complement and substantiate our findings. This study was registered with PROSPERO as CRD 42024527587.
Keywords: dietary pattern; lifestyle modification; medical nutrition therapy; perinatal complications; physical activity.
Copyright © 2024 The Author(s). Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Conflict of interest The authors report no conflicts of interest.
Figures
References
-
- Guariguata L., Linnenkamp U., Beagley J., Whiting D.R., Cho N.H. Global estimates of the prevalence of hyperglycaemia in pregnancy. Diabetes Res. Clin. Pract. 2014;103(2):176–185. - PubMed
-
- Ferrara A. Increasing prevalence of gestational diabetes mellitus: a public health perspective. Diabetes Care. 2007;30(Suppl 2):S141–S146. - PubMed
-
- Gregory E.C., Ely D.M. Trends and characteristics in gestational diabetes: United States, 2016-2020. Natl. Vital. Stat. Rep. 2022;71(3):1–15. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
