

Semaglutide normalizes increased cardiomyocyte calcium transients in a rat model of high fat diet-induced obesity
- PMID: 39482267
- PMCID: PMC11911617
- DOI: 10.1002/ehf2.15152
Semaglutide normalizes increased cardiomyocyte calcium transients in a rat model of high fat diet-induced obesity
Abstract
Aims: Obesity increases the risk of heart failure with preserved (HFpEF), but not reduced ejection fraction (HFrEF). The glucagon-like peptide-1 receptor agonist (GLP-1-RA) semaglutide improves outcome of patients with obesity with or without HFpEF, while GLP-1-RAs were associated with adverse outcome in patients with HFrEF. Here, we investigate the effect of in vivo treatment with semaglutide on excitation-contraction coupling in a rat model of obesity.
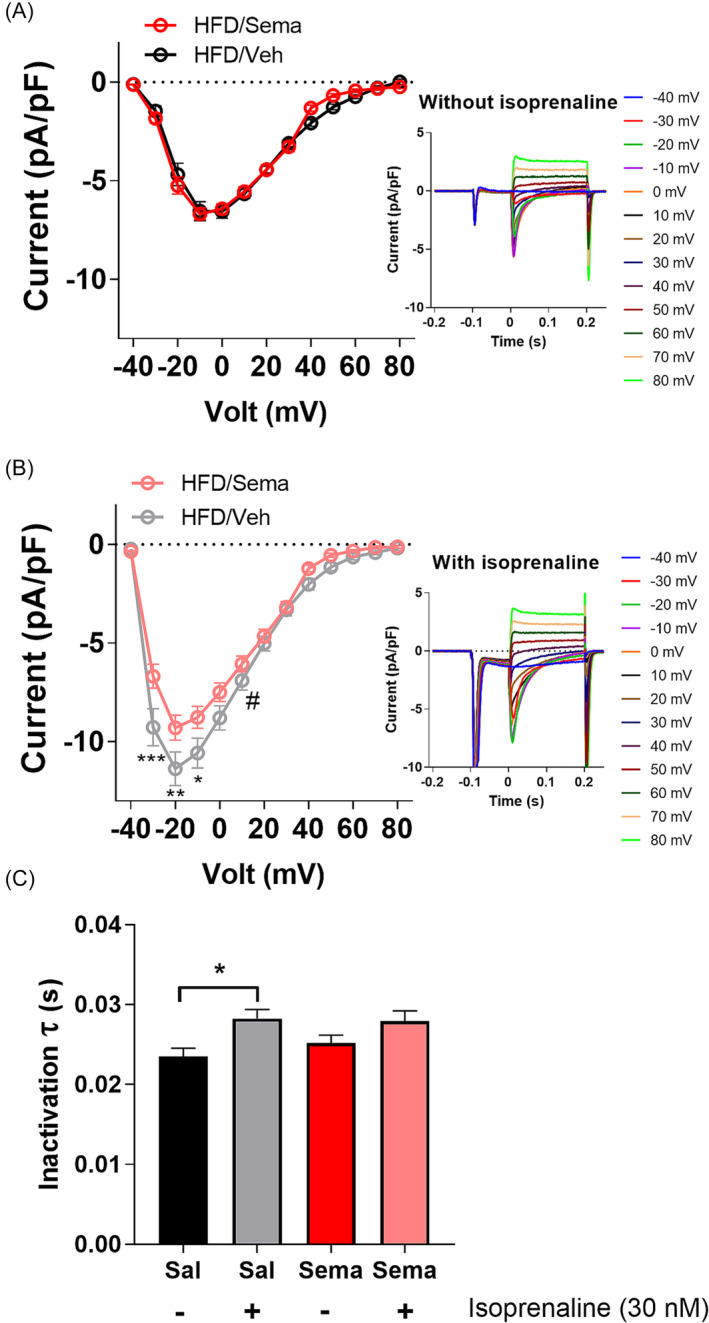
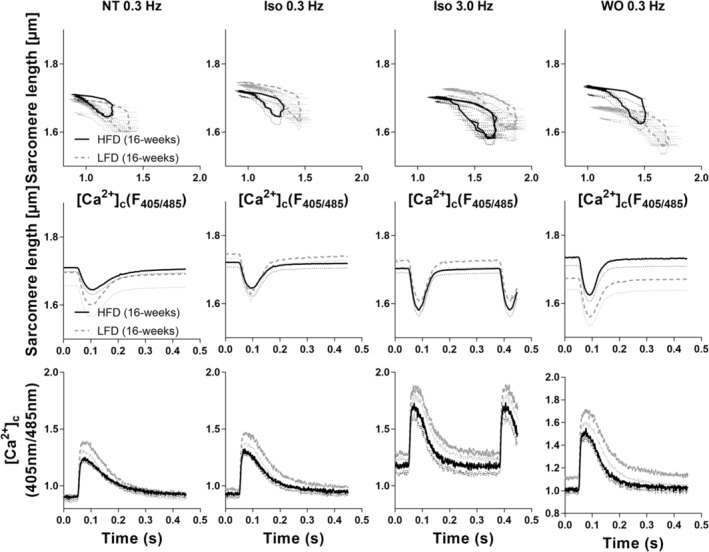
Methods and results: Rats received high-fat/high-fructose diet for 8 weeks and were then randomized to semaglutide (HFD/Sema) or vehicle (HFD/Veh) for another 8 weeks, during which they could choose between HFD and a low-fat/high-fructose diet (LFD). Control rats received either standard chow (CON), HFD or LFD only, without treatment. After 16 weeks, sarcomere shortening and cytosolic Ca2+ concentrations ([Ca2+]c) were determined in isolated cardiomyocytes. Compared with CON, HFD/Veh increased the amplitude of [Ca2+]c transients and systolic sarcomere shortening in absence or presence of β-adrenergic stimulation, which was reversed by HFD/Sema. Caffeine-induced sarcoplasmic reticulum (SR) Ca2+ release and L-type Ca2+ channel (LTCC) currents were reduced by HFD/Sema versus HFD/Veh, while SR Ca2+ ATPase activity remained unaffected. Compared with HFD, LFD increased [Ca2+]c transients and sarcomere shortening further despite similar effects on body weight.
Conclusions: While HFD increased cardiomyocyte [Ca2+]c transients and systolic sarcomere shortening, semaglutide normalized these alterations, mediated by reduced SR Ca2+ load and LTCC currents. Because increased LTCC currents were previously traced to cardiac hypertrophy, these effects may explain why GLP-1-RAs provide benefits for patients with obesity with or without HFpEF, but rather adverse outcome in HFrEF.
Keywords: Excitation‐contraction coupling; Glucagon‐like peptide agonists; Heart failure; Obesity; Semaglutide.
© 2024 The Author(s). ESC Heart Failure published by John Wiley & Sons Ltd on behalf of European Society of Cardiology.
Conflict of interest statement
C.M. received speaker or advisory honoraria from Bristol Myers Squibb, Boehringer Ingelheim, AstraZeneca, Servier, Amgen, NovoNordisk, Bayer, Novartis, Edwards and Berlin Chemie. U.D. has received speaker honoraria of Alnylam, Recordati Rare Diseases and MSD. All other authors have declared that no conflict of interest exists.
Figures





References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
