

Intersecting social and environmental determinants of multidrug-resistant urinary tract infections in East Africa beyond antibiotic use
- PMID: 39482320
- PMCID: PMC11528027
- DOI: 10.1038/s41467-024-53253-x
Intersecting social and environmental determinants of multidrug-resistant urinary tract infections in East Africa beyond antibiotic use
Abstract
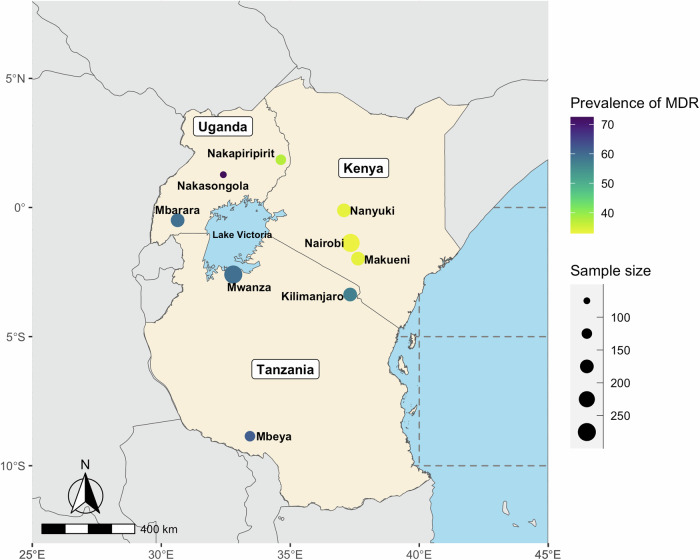
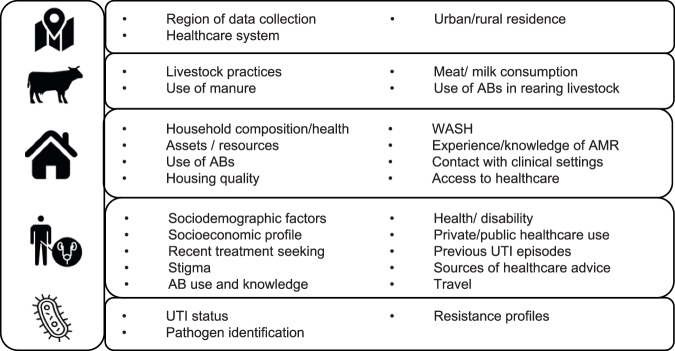
The global health crisis of antibacterial resistance (ABR) poses a particular threat in low-resource settings like East Africa. Interventions for ABR typically target antibiotic use, overlooking the wider set of factors which drive vulnerability and behaviours. In this cross-sectional study, we investigated the joint contribution of behavioural, environmental, socioeconomic, and demographic factors associated with higher risk of multi-drug resistant urinary tract infections (MDR UTIs) in Kenya, Tanzania, and Uganda. We sampled outpatients with UTI symptoms in healthcare facilities and linked their microbiology data with patient, household and community level data. Using bivariate statistics and Bayesian profile regression on a sample of 1610 individuals, we show that individuals with higher risk of MDR UTIs were more likely to have compound and interrelated social and environmental disadvantages: they were on average older, with lower education, had more chronic illness, lived in resource-deprived households, more likely to have contact with animals, and human or animal waste. This suggests that interventions to tackle ABR need to take account of intersectional socio-environmental disadvantage as a priority.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures




References
-
- O’Neill, J. Antimicrobial Resistance: Tackling a Crisis for the Health and Wealth of Nations. (Rev. Antimicrob. Resist., 2014).
Publication types
MeSH terms
Substances
Grants and funding
- MR/S004785/1/RCUK | Medical Research Council (MRC)
- MR/S004785/1/RCUK | Medical Research Council (MRC)
- MR/S004785/1/RCUK | Medical Research Council (MRC)
- MR/S004785/1/RCUK | Medical Research Council (MRC)
- MR/S004785/1/RCUK | Medical Research Council (MRC)
- MR/S004785/1/RCUK | Medical Research Council (MRC)
- MR/S004785/1/RCUK | Medical Research Council (MRC)
- MR/S004785/1/RCUK | Medical Research Council (MRC)
- MR/S004785/1/RCUK | Medical Research Council (MRC)
- MR/S004785/1/RCUK | Medical Research Council (MRC)
- MR/S004785/1/RCUK | Medical Research Council (MRC)
- MR/S004785/1/RCUK | Medical Research Council (MRC)
- GCRF Consolidator Award/Scottish Funding Council (SFC)
- GCRF Consolidator Award/Scottish Funding Council (SFC)
- MR/S004785/1/RCUK | MRC | Medical Research Foundation
- MR/S004785/1/RCUK | MRC | Medical Research Foundation
- MR/S004785/1/RCUK | MRC | Medical Research Foundation
- U01CA207167/Foundation for the National Institutes of Health (Foundation for the National Institutes of Health, Inc.)
LinkOut - more resources
Full Text Sources
Medical
