

High-throughput Bronchus-on-a-Chip system for modeling the human bronchus
- PMID: 39482373
- PMCID: PMC11528030
- DOI: 10.1038/s41598-024-77665-3
High-throughput Bronchus-on-a-Chip system for modeling the human bronchus
Abstract
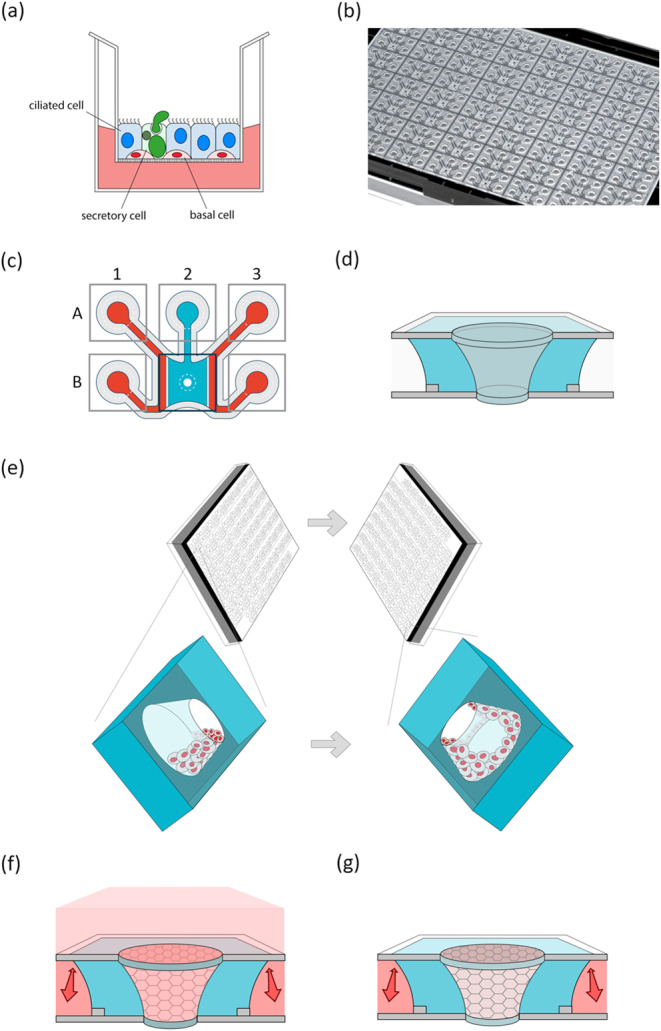
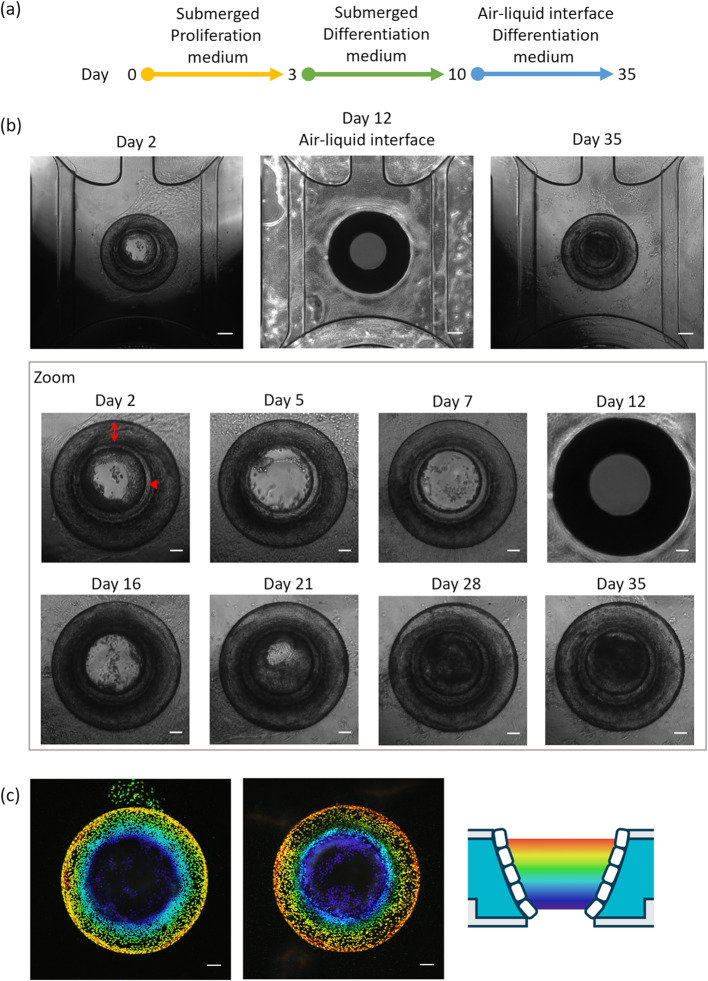
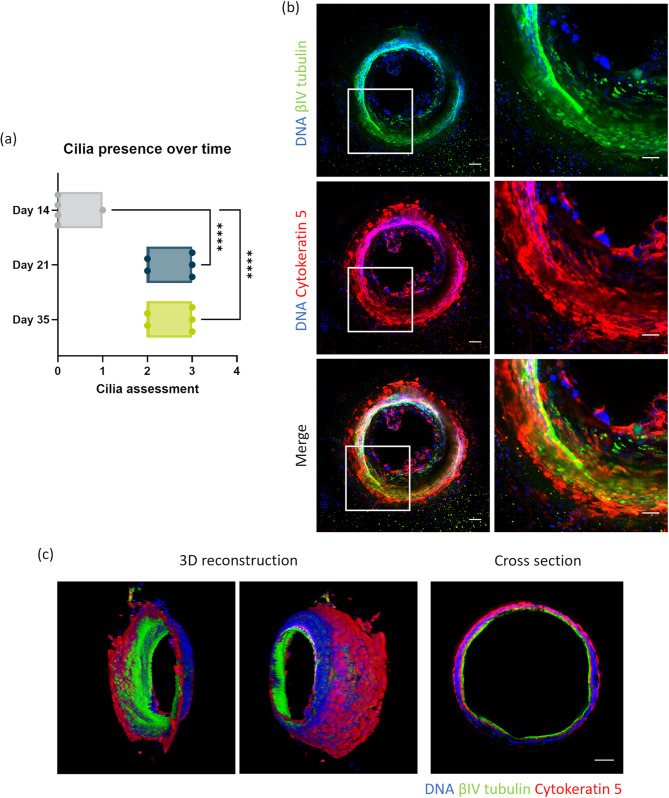
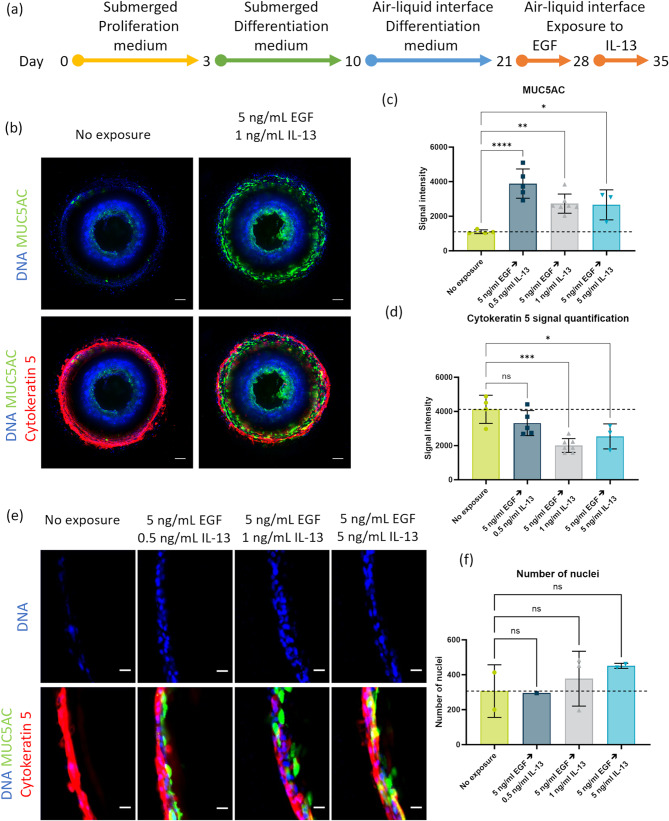
Airway inflammation, a protective response in the human body, can disrupt normal organ function when chronic, as seen in chronic obstructive pulmonary disease (COPD) and asthma. Chronic bronchitis induces goblet cell hyperplasia and metaplasia, obstructing airflow. Traditional animal testing is often replaced by in vitro three-dimensional cultures of human epithelial cells to assess chronic cell responses. However, these cells are cultured horizontally, differing from the tubular structure of the human airway and failing to accurately reproduce airway stenosis. To address this, we developed the Bronchus-on-a-Chip (BoC) system. The BoC uses a novel microfluidic design in a standard laboratory plate, embedding 62 chips in one plate. Human bronchial epithelial cells were cultured against a collagen extracellular matrix for up to 35 days. Characterization included barrier integrity assays, microscopy, and histological examination. Cells successfully cultured in a tubular structure, with the apical side air-lifted. Epithelial cells differentiated into basal, ciliated, and secretory cells, mimicking human bronchial epithelium. Upon exposure to inducers of goblet cell hyperplasia and metaplasia, the BoC system showed mucus hyperproduction, replicating chronic epithelial responses. This BoC system enhances in vitro testing for bronchial inflammation, providing a more human-relevant and high-throughput method.
Keywords: 3D-reconstructed airway epithelial cells; Airway-on-a-chip; Organotypic culture.
© 2024. The Author(s).
Conflict of interest statement
Mimetas B.V. markets the OrganoPlate®. Execution of this work was supported by funding of Japan Tobacco Inc. AM, KM, KO, and SI are employees of Japan Tobacco Inc., and MV, LB, JH, AN, JB, TB, and BK are employees of Mimetas B.V.
Figures

References
-
- ICRP, Annals of the ICRP. Human Respiratory Tract Model for Radiological Protection, ed. I.P. 66. Vol. 24. (1994). - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
