

IFSO Bariatric Endoscopy Committee Evidence-Based Review and Position Statement on Endoscopic Sleeve Gastroplasty for Obesity Management
- PMID: 39482444
- PMCID: PMC11671576
- DOI: 10.1007/s11695-024-07510-z
IFSO Bariatric Endoscopy Committee Evidence-Based Review and Position Statement on Endoscopic Sleeve Gastroplasty for Obesity Management
Erratum in
-
Correction: IFSO Bariatric Endoscopy Committee Evidence-Based Review and Position Statement on Endoscopic Sleeve Gastroplasty for Obesity Management.Obes Surg. 2024 Dec;34(12):4349. doi: 10.1007/s11695-024-07580-z. Obes Surg. 2024. PMID: 39546177 Free PMC article. No abstract available.
Abstract
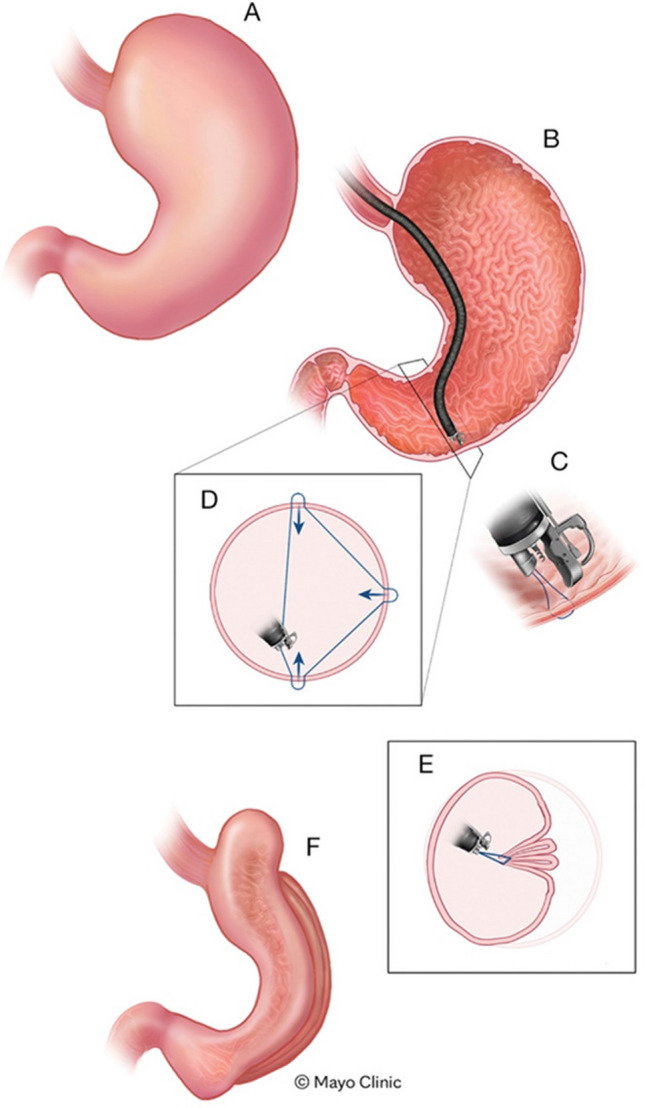
Background: Obesity is a significant global health issue. Metabolic and bariatric surgery (MBS) is the gold standard in the treatment of obesity due to its proven effectiveness and safety in the short and long term. However, MBS is not suitable for all patients. Some individuals are at high surgical risk or refuse surgical treatment, while others do not meet the criteria for MBS despite having obesity-related comorbidities. This gap has driven the development of endoscopic solutions like endoscopic sleeve gastroplasty (ESG), which offers a less invasive alternative that preserves organ function and reduces risks. A recent IFSO International Delphi consensus study highlighted that multidisciplinary experts agree on the utility of ESG for managing obesity in patients with class I and II obesity and for those with class III obesity who do not wish to pursue or qualify for MBS. This IFSO Bariatric Endoscopy Committee position statement aims to augment these consensus statements by providing a comprehensive systematic review of the evidence and delivering an evidence-based position on the value of ESG within the spectrum of obesity management.
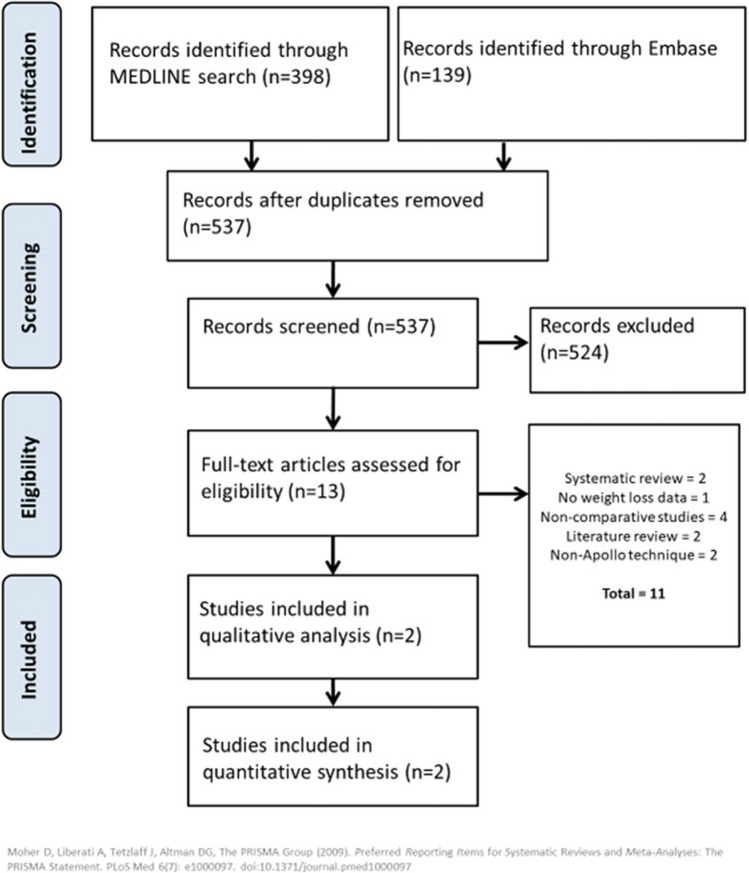
Methods: A comprehensive systematic review followed the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) and Cochrane guidelines.
Results: Systematic Review: The systematic review included 44 articles encompassing 15,714 patients receiving ESG. The studies varied from large case series to cohort studies and a randomized controlled trial (RCT). The mean baseline BMI was 37.56 kg/m2. The review focused on weight loss outcomes and safety data.
Meta-analysis: Time point Mean %EWL Mean %TBWL 6 months 48.04 15.66 12 months 53.09 17.56 18 months 57.98 16.25 24 months 46.57 15.2 36 months 53.18 14.07 60 months 45.3 15.9 These results demonstrate significant weight loss following ESG.
Safety: The pooled serious adverse event (SAE) rate was 1.25%. This low rate of SAEs indicates that ESG is a relatively safe procedure.
Quality of evidence: The quality of evidence from the included observational studies was assessed as very low, primarily due to the inherent limitations associated with observational study designs, such as potential biases and lack of randomization. In contrast, the quality of evidence from the single randomized controlled trial was rated as MODERATE, reflecting a more robust study design that provides a higher level of evidence despite some limitations.
Conclusions: The IFSO Bariatric Endoscopy Committee, after conducting a comprehensive systematic review and meta-analysis, endorses endoscopic sleeve gastroplasty (ESG) as an effective and valuable treatment for obesity. ESG is particularly beneficial for patients with class I and II obesity, as well as for those with class III obesity who are not suitable candidates for metabolic bariatric surgery. ESG provides significant weight loss outcomes and demonstrates a favorable safety profile with a low rate of serious adverse events. Despite the limitations of the included observational studies, the randomized controlled trial included in the analysis reinforces the efficacy and safety of ESG and provides an evidence-based foundation for the position statement. Thus, the IFSO position statement supports and provides an evidence base for the role of ESG within the broader spectrum of obesity management.
Keywords: Endoscopic Sleeve Gastroplasty; Meta-analysis; Obesity.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Competing Interests: Barham K. Abu Dayyeh: Received research support and educational consulting fees from Boston Scientific; previously Apollo Endosurgery. Additionally, received research support from USGI Medical. Christine Stier: Consulting and educational engagements with Boston Scientific. Aayed Alqahtani: Consulting and educational engagements with Boston Scientific. Reem Sharaiha: Consulting and educational engagements with Boston Scientific. Mohit Bandhari: Consulting and educational engagements with Boston Scientific. Silvana Perretta: Consulting and educational engagements with Boston Scientific. Sigh Pichamol Jirapinyo: Consulting and educational engagements with Boston Scientific. Gerhard Prager: Declares no conflicts of interest related to this study. Ricardo Cohen: Declares no conflicts of interest related to this study.
Figures





References
-
- World Healh Organization. Overweight and obesity - global observatory data. https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight.
-
- Hales CM, Carroll MD, Fryar CD, et al. Prevalence of obesity among adults and youth: United States, 2015–2016. NCHS Data Brief. 2017;288:1–8. - PubMed
-
- Finkelstein EA, Khavjou OA, Thompson H, et al. Obesity and severe obesity forecasts through 2030. Am J Prev Med. 2012;42:563–70. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
