

Proteogenomic analysis dissects early-onset breast cancer patients with prognostic relevance
- PMID: 39482530
- PMCID: PMC11612404
- DOI: 10.1038/s12276-024-01332-w
Proteogenomic analysis dissects early-onset breast cancer patients with prognostic relevance
Abstract
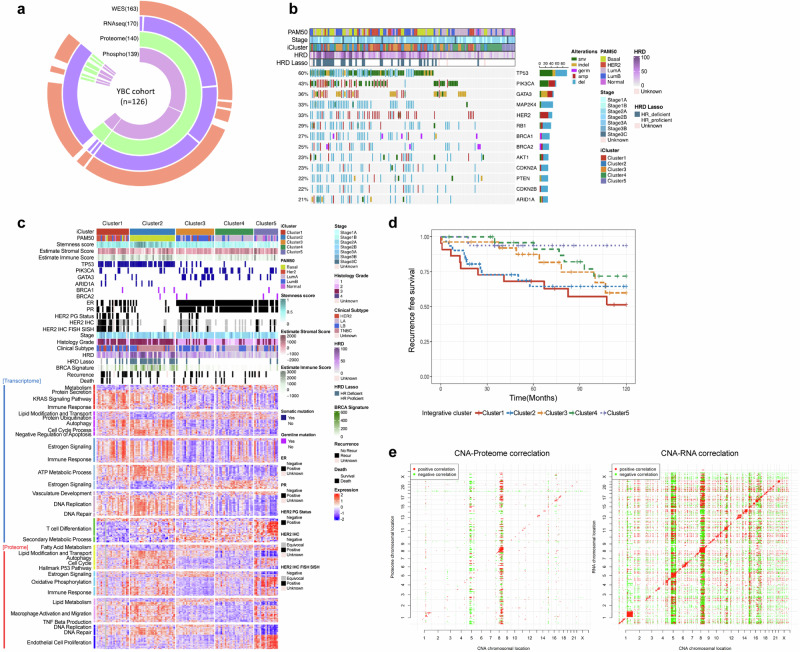
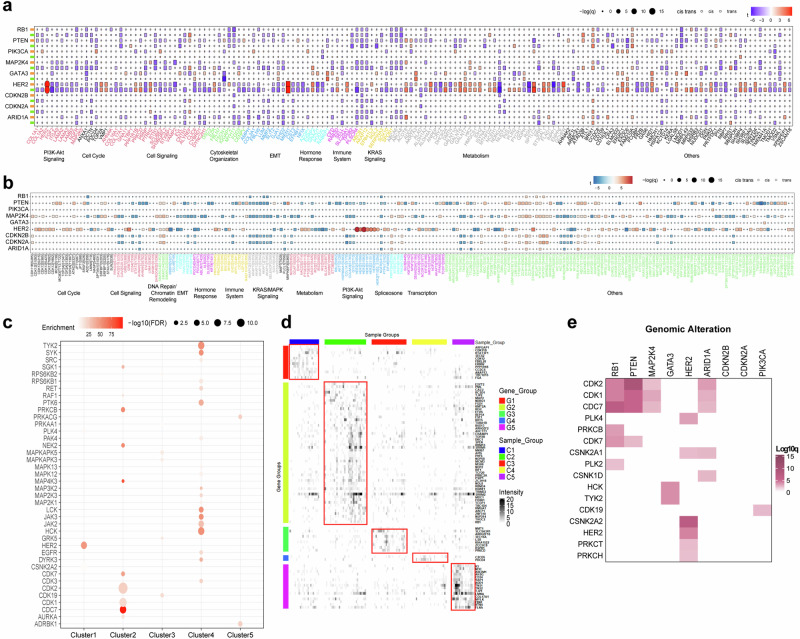
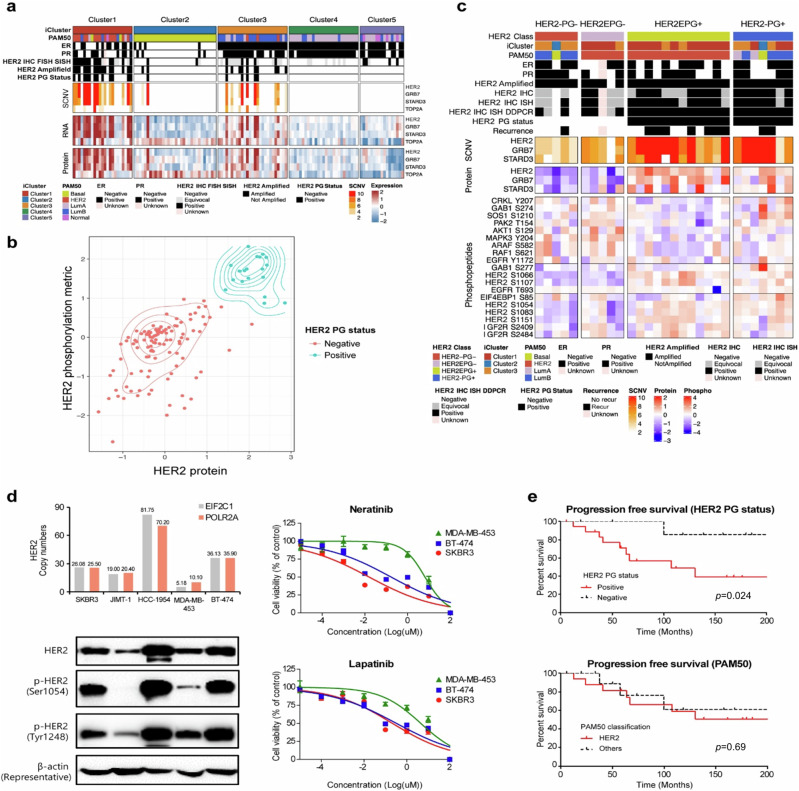
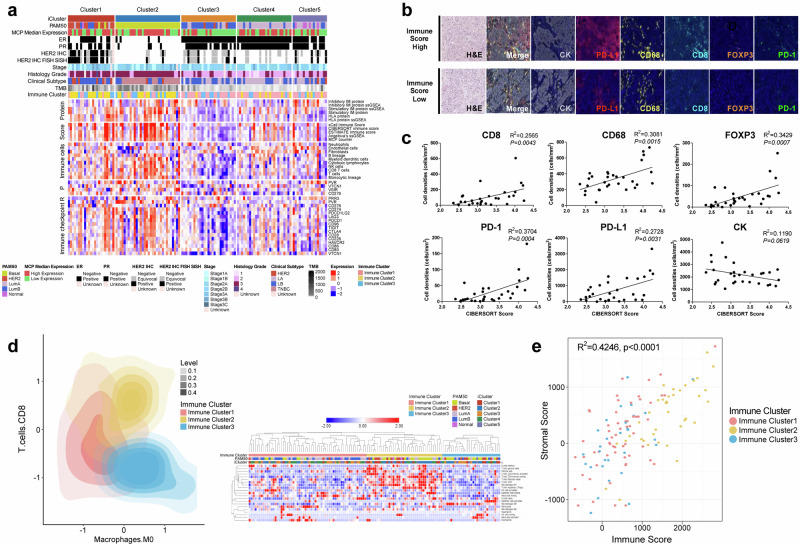
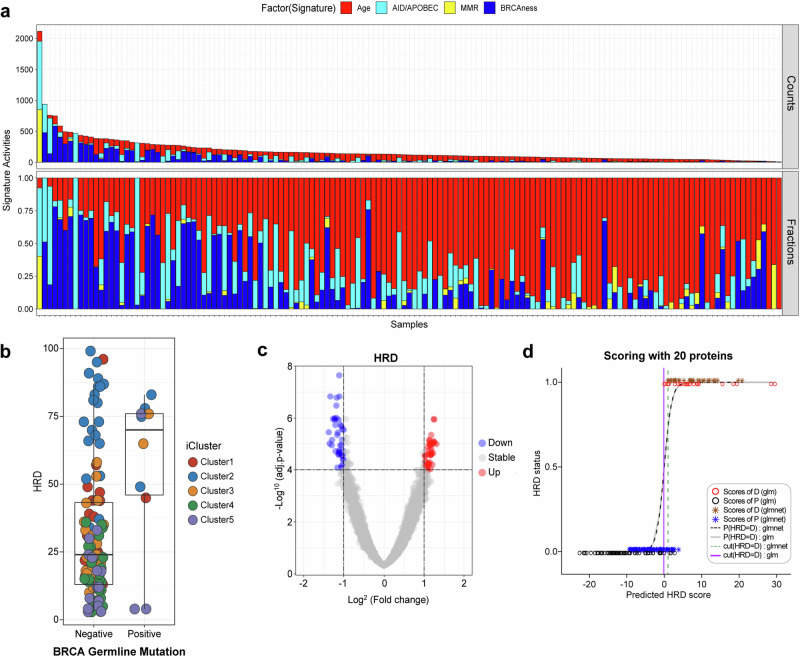
Early-onset breast cancer is known for its aggressive clinical characteristics and high prevalence in East Asian countries, but a comprehensive understanding of its molecular features is still lacking. In this study, we conducted a proteogenomic analysis of 126 treatment-naïve primary tumor tissues obtained from Korean patients with young breast cancer (YBC) aged ≤40 years. By integrating genomic, transcriptomic, and proteomic data, we identified five distinct functional subgroups that accurately represented the clinical characteristics and biological behaviors of patients with YBC. Our integrated approach could be used to determine the proteogenomic status of HER2, enhancing its clinical significance and prognostic value. Furthermore, we present a proteome-based homologous recombination deficiency (HRD) analysis that has the potential to overcome the limitations of conventional genomic HRD tests, facilitating the identification of new patient groups requiring targeted HR deficiency treatments. Additionally, we demonstrated that protein-RNA correlations can be used to predict the late recurrence of hormone receptor-positive breast cancer. Within each molecular subtype of breast cancer, we identified functionally significant protein groups whose differential abundance was closely correlated with the clinical progression of breast cancer. Furthermore, we derived a recurrence predictive index capable of predicting late recurrence, specifically in luminal subtypes, which plays a crucial role in guiding decisions on treatment durations for YBC patients. These findings improve the stratification and clinical implications for patients with YBC by contributing to the optimal adjuvant treatment and duration for favorable clinical outcomes.
© 2024. The Author(s).
Conflict of interest statement
Competing interests: J.K. is an employee of GSK, USA, and the other authors declare no competing interests.
Figures
References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
