

Body posture can modulate liver stiffness measured by transient elastography: a prospective observational study
- PMID: 39482593
- PMCID: PMC11526721
- DOI: 10.1186/s12876-024-03473-8
Body posture can modulate liver stiffness measured by transient elastography: a prospective observational study
Abstract
Background: Non-invasive measurement of liver stiffness (LS), traditionally performed in the supine position, has been established to assess liver fibrosis. However, fibrosis degree is not the sole determinant of LS, necessitating the identification of relevant confounders. One often-overlooked factor is body posture, and it remains unclear whether normal daily postures interfere with LS irrespective of fibrosis. A prospective two-group comparison study was conducted to investigate the relationship between posture and LS.
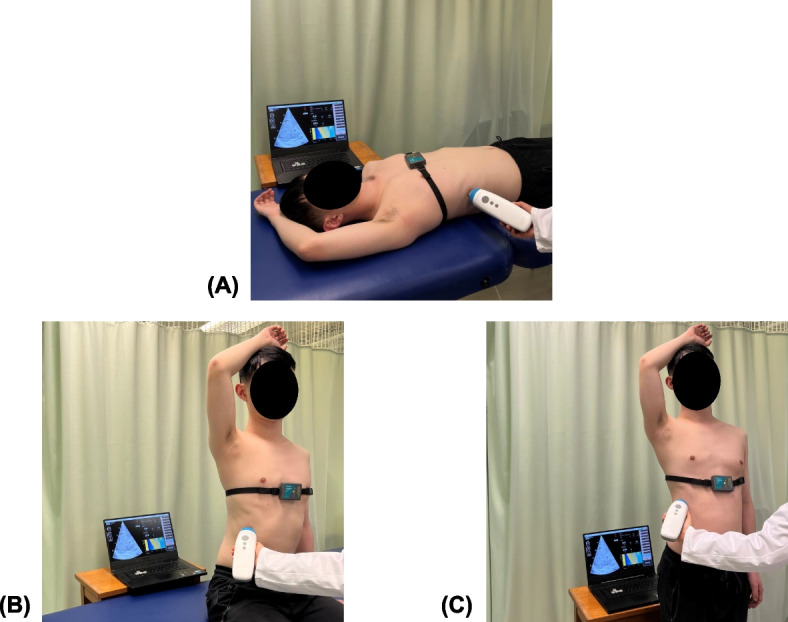
Methods: Sixty-two adults participated, divided into two groups: patients with chronic liver disease and healthy controls. Both groups were assessed using transient elastography (TE) under the supine, seated, and standing postures. Randomization was applied to the order of the two upright postures. A two-way mixed ANOVA was conducted to assess the posture-dependence of LS and its variations between two groups.
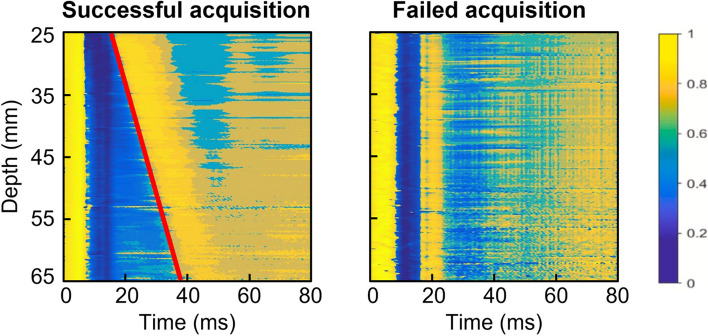
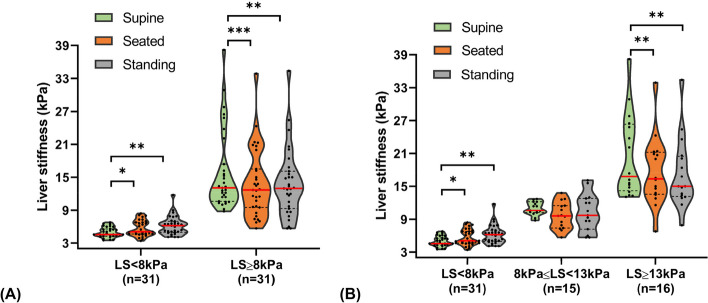
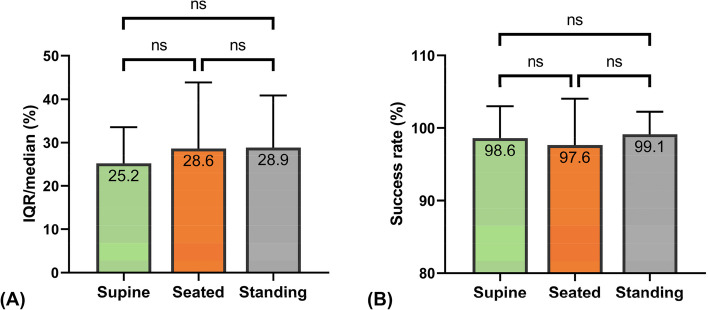
Results: Results showed that posture differentially affected LS depending on the presence of liver fibrosis. In 31 healthy individuals (baseline LS range: 3.5-6.8 kPa), a transition from the supine (5.0 ± 1.0 kPa) to seated (5.7 ± 1.4 kPa; p = 0.036) or standing (6.2 ± 1.7 kPa; p = 0.002) positions increased LS, indicating liver stiffening. Conversely, in 31 patients with varying fibrosis stages (baseline LS range: 8.8-38.2 kPa), posture decreased LS from the supine (15.9 ± 7.3 kPa) to seated (13.8 ± 6.2 kPa; p < 0.001) or standing (13.9 ± 6.2 kPa; p = 0.001) positions. No significant difference in LS was observed between the seated and standing positions in both groups (control group: 5.7 vs. 6.2 kPa, p = 0.305; patient group: 13.8 vs. 13.9 kPa, p = 1). Additionally, different postures did not elicit significant changes in the success rate (supine, 98.6 ± 4%; seated, 97.6 ± 6%; standing, 99.1 ± 3%; p = 0.258) and IQR/median value (supine, 25 ± 8%; seated, 29 ± 15%; standing, 29 ± 12%; p = 0.117), implying no impact on both measurement feasibility and reliability.
Conclusions: We demonstrated, for the first time, the feasibility of utilizing upright postures as an alternative measurement protocol for TE. We further unravel a previously unrecognized role of transitioning between different postures to assist the diagnosis of cirrhosis. The findings suggested that daily physiological activity of postural changes suffices to alter LS. Therefore, body positioning should be standardized and carefully considered when interpreting LS.
Keywords: Body position; Liver fibrosis; Liver stiffness measurement; Measuring posture; Patient positioning; Ultrasound elastography.
© 2024. The Author(s).
Conflict of interest statement
Y.L. is currently a full-time employee of Eieling Technology Limited. M.-H.Z. has received honoraria for lectures from AstraZeneca, Hisky Medical Technologies, and Novo Nordisk and consulting fee from Boehringer Ingelheim. Y.-P.Z. serves as the advisory board member for Eieling Technology Limited via his home university of The Hong Kong Polytechnic University. The other authors declare have no competing interests.
Figures
Similar articles
-
Normal liver stiffness in healthy adults assessed by real-time shear wave elastography and factors that influence this method.Ultrasound Med Biol. 2014 Nov;40(11):2549-55. doi: 10.1016/j.ultrasmedbio.2014.05.008. Ultrasound Med Biol. 2014. PMID: 25282481
-
Which are the cut-off values of 2D-Shear Wave Elastography (2D-SWE) liver stiffness measurements predicting different stages of liver fibrosis, considering Transient Elastography (TE) as the reference method?Eur J Radiol. 2014 Mar;83(3):e118-22. doi: 10.1016/j.ejrad.2013.12.011. Epub 2013 Dec 17. Eur J Radiol. 2014. PMID: 24380640
-
Comparison between ROI-based and volumetric measurements in quantifying heterogeneity of liver stiffness using MR elastography.Eur Radiol. 2020 Mar;30(3):1609-1615. doi: 10.1007/s00330-019-06478-0. Epub 2019 Nov 8. Eur Radiol. 2020. PMID: 31705257
-
Comparison of point shear wave elastography and transient elastography in the evaluation of patients with NAFLD.Radiol Med. 2022 May;127(5):571-576. doi: 10.1007/s11547-022-01475-8. Epub 2022 Mar 15. Radiol Med. 2022. PMID: 35290569
-
When the liver gets stiff, the tough get moving.J Gastroenterol Hepatol. 2020 Jun;35(6):953-959. doi: 10.1111/jgh.14963. Epub 2020 Feb 11. J Gastroenterol Hepatol. 2020. PMID: 31867782 Review.
Cited by
-
Non-Invasive Tests as a Replacement for Liver Biopsy in the Assessment of MASLD.Medicina (Kaunas). 2025 Apr 16;61(4):736. doi: 10.3390/medicina61040736. Medicina (Kaunas). 2025. PMID: 40283027 Free PMC article. Review.
References
-
- Rockey DC, Caldwell SH, Goodman ZD, Nelson RC, Smith AD. Liver biopsy. Hepatology (Baltimore, MD). 2009;49(3):1017–44. - PubMed
-
- Sandrin L, Fourquet B, Hasquenoph J-M, Yon S, Fournier C, Mal F, et al. Transient elastography: a new noninvasive method for assessment of hepatic fibrosis. Ultrasound Med Biol. 2003;29(12):1705–13. - PubMed
-
- Who. Guidelines for the Prevention Care and Treatment of Persons with Chronic Hepatitis B Virus Infection: Mar-15. 1 ed. Geneva: World Health Organization; 2015. - PubMed
-
- Shiha G, Ibrahim A, Helmy A, Sarin SK, Omata M, Kumar A, et al. Asian-Pacific Association for the Study of the Liver (APASL) consensus guidelines on invasive and non-invasive assessment of hepatic fibrosis: a 2016 update. Hep Intl. 2017;11(1):1–30. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
