

Long COVID and the Autonomic Nervous System: The Journey from Dysautonomia to Therapeutic Neuro-Modulation through the Retrospective Analysis of 152 Patients
- PMID: 39483361
- PMCID: PMC11523758
- DOI: 10.3390/neurosci3020021
Long COVID and the Autonomic Nervous System: The Journey from Dysautonomia to Therapeutic Neuro-Modulation through the Retrospective Analysis of 152 Patients
Abstract
Introduction: The severity and prevalence of Post-Acute COVID-19 Sequela (PACS) or long-COVID syndrome (long COVID) should not be a surprise. Long-COVID symptoms may be explained by oxidative stress and parasympathetic and sympathetic (P&S) dysfunction. This is a retrospective, hypothesis generating, outcomes study.
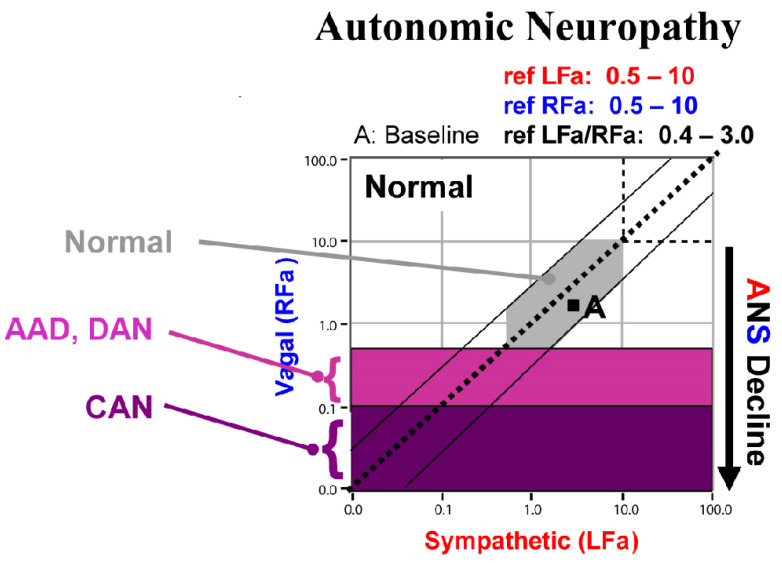
Methods: From two suburban practices in northeastern United States, 152 long COVID patients were exposed to the following practices: (1) first, they were P&S tested (P&S Monitor 4.0; Physio PS, Inc., Atlanta, GA, USA) prior to being infected with COVID-19 due to other causes of autonomic dysfunction; (2) received a pre-COVID-19 follow-up P&S test after autonomic therapy; (3) then, they were infected with COVID-19; (4) P&S tested within three months of surviving the COVID-19 infection with long-COVID symptoms; and, finally, (5) post-COVID-19, follow-up P&S tested, again, after autonomic therapy. All the patients completed autonomic questionnaires with each test. This cohort included 88 females (57.8%), with an average age of 47.0 years (ranging from 14 to 79 years), and an average BMI of 26.9 #/in2.
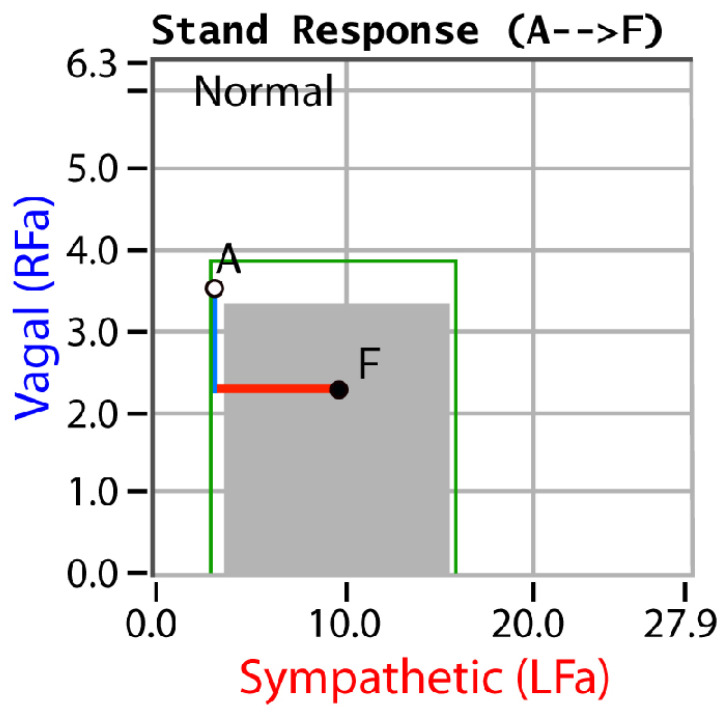
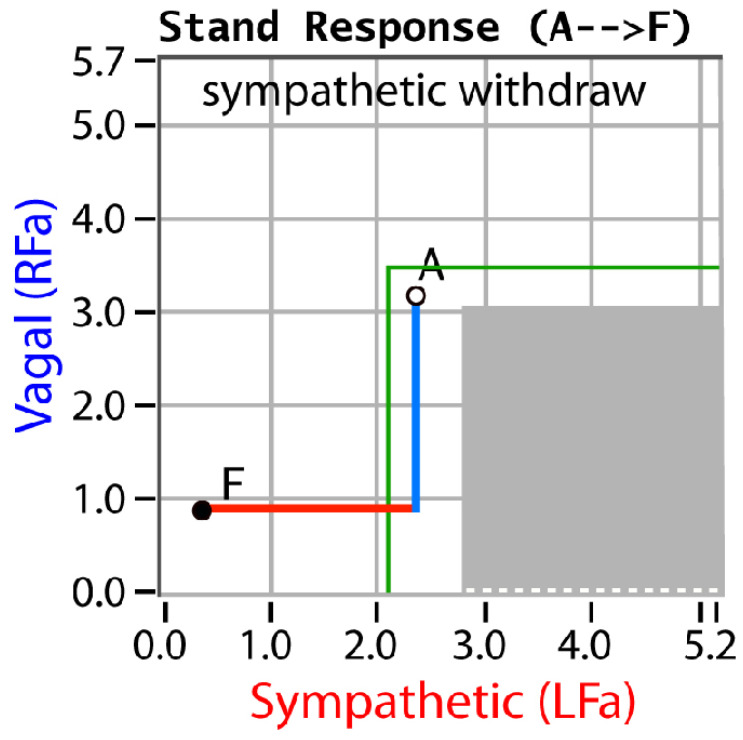
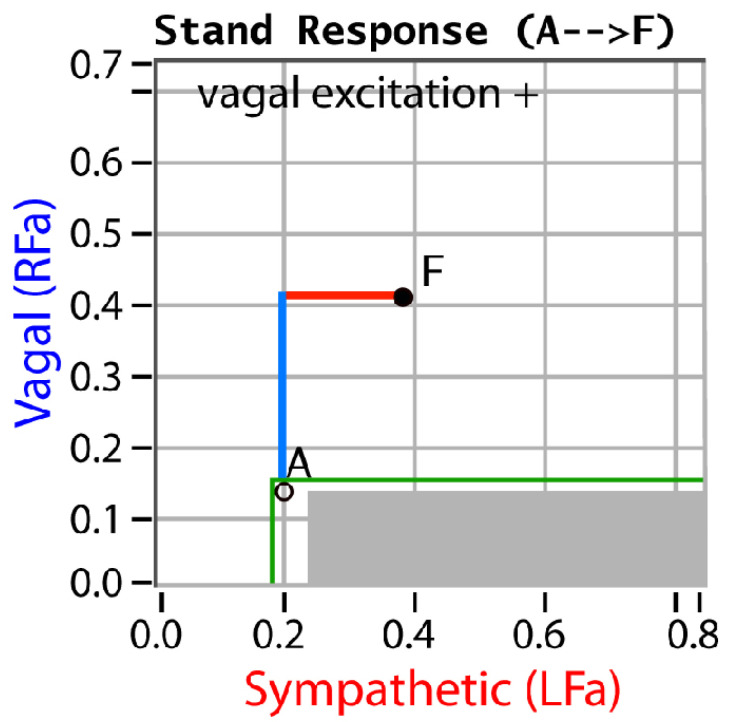
Results: More pre-COVID-19 patients presented with sympathetic withdrawal than parasympathetic excess. Post-COVID-19, these patients presented with this ratio reversed and, on average, 49.9% more autonomic symptoms than they did pre-COVID-19.
Discussion: Both parasympathetic excess and sympathetic withdrawal are separate and treatable autonomic dysfunctions and autonomic treatment significantly reduces the prevalence of autonomic symptoms.
Conclusion: SARS-CoV-2, via its oxidative stress, can lead to P&S dysfunction, which, in turn, affects the control and coordination of all systems throughout the whole body and may explain all of the symptoms of long-COVID syndrome. Autonomic therapy leads to positive outcomes and patient quality of life may be restored.
Keywords: autonomic dysfunction; autonomic therapy; long COVID; outcomes; parasympathetic; sympathetic.
© 2022 by the authors.
Conflict of interest statement
Conflicts of InterestOnly Colombo has a conflict of interest as Co-Founder and Sr. Medical Director of Physio PS, Inc. No other individual associated with this manuscript has a conflict of interest.
Figures
References
-
- DePace N.L., Colombo J. Long-covid syndrome: A multi-organ disorder. Cardio. Open. 2022;7:212–223.
-
- DePace N.L., Colombo J. Long-COVID syndrome: A review of what we have learned clinically to date. 2022. Submitted .
-
- DePace N.L., Colombo J. Autonomic and Mitochondrial Dysfunction in Clinical Diseases: Diagnostic, Prevention, and Therapy. Springer Science + Business Media; New York, NY, USA: 2019.
-
- Colombo J., Arora R.R., DePace N.L., Vinik A.I. Clinical Autonomic Dysfunction: Measurement, Indications, Therapies, and Outcomes. Springer Science + Business Media; New York, NY, USA: 2014.
LinkOut - more resources
Full Text Sources
Miscellaneous
