

Optimal timing of percutaneous coronary intervention in elderly patients with acute ST-segment elevation myocardial infarction presenting late
- PMID: 39484103
- PMCID: PMC11523474
- DOI: 10.5114/kitp.2024.143685
Optimal timing of percutaneous coronary intervention in elderly patients with acute ST-segment elevation myocardial infarction presenting late
Abstract
Introduction: Primary percutaneous coronary intervention (PPCI) is an effective method for the clinical treatment of acute ST-segment elevation myocardial infarction (STEMI). For patients who miss the optimal time window, optimal management of these patients remains controversial.
Aim: To compare the effects of different timing of percutaneous coronary intervention on the long-term prognosis of elderly patients with acute ST-segment elevation myocardial infarction (STEMI) with time from symptom onset > 12 hours.
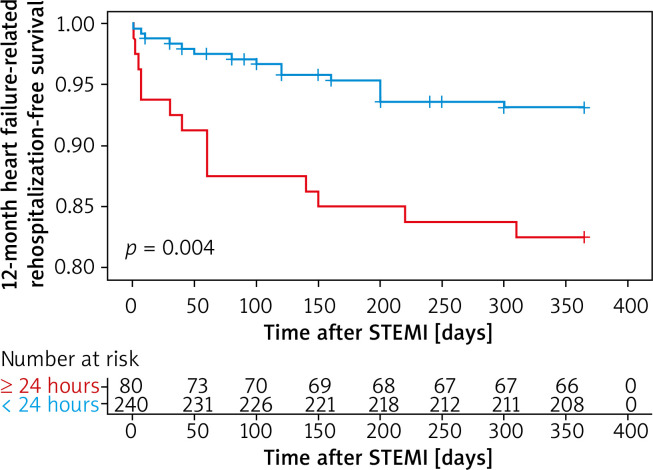
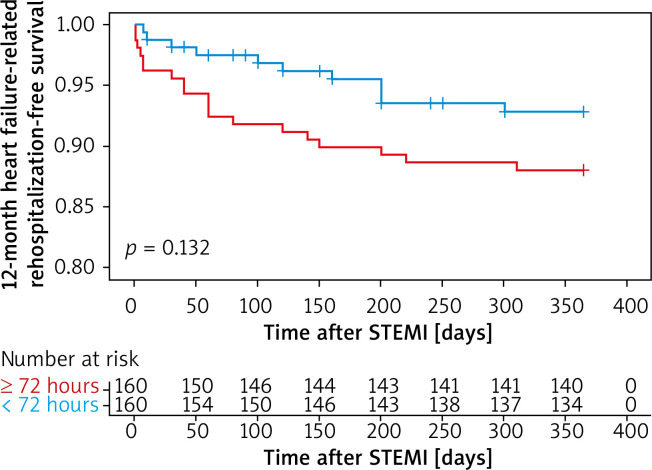
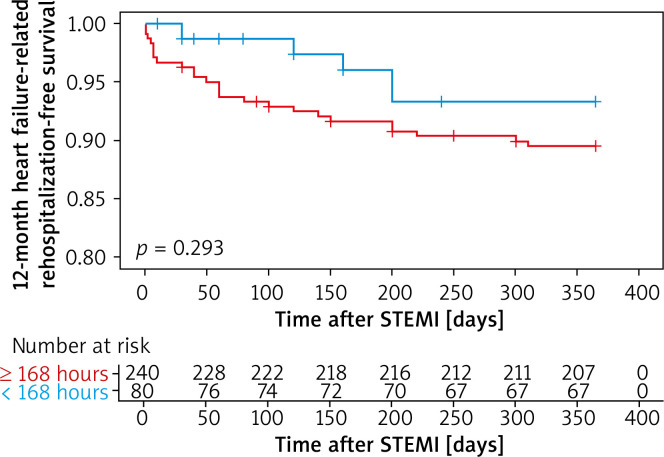
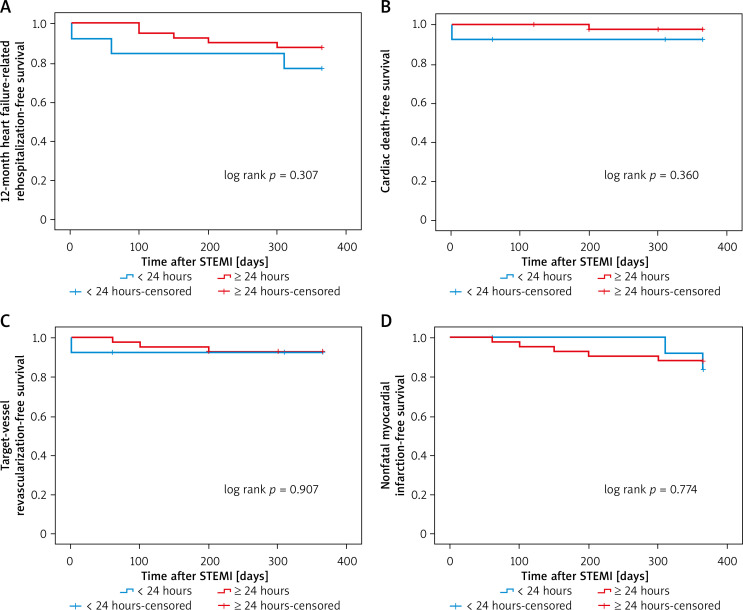
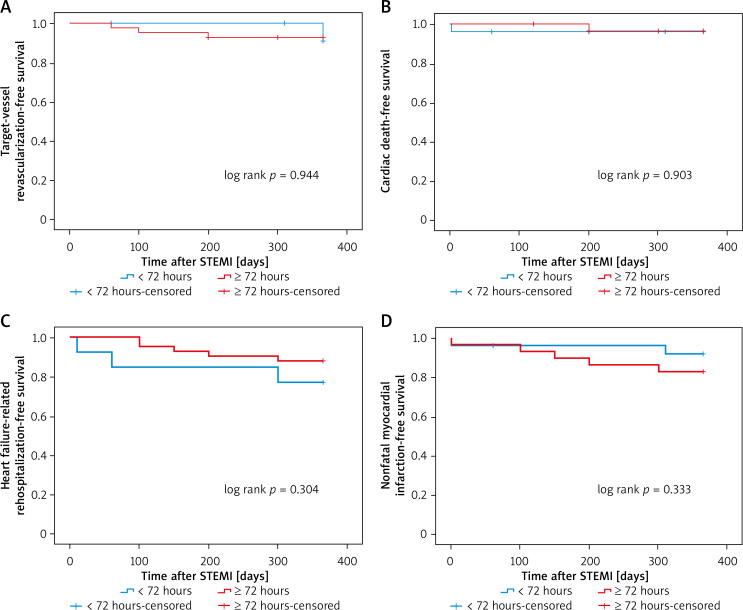
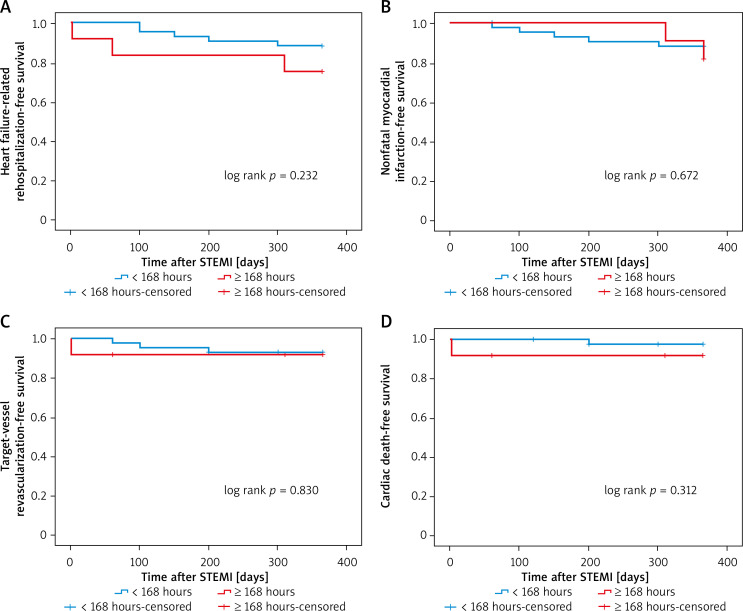
Material and methods: Elderly acute STEMI patients with time from symptom onset > 12 hours in the period from July 2021 to July 2022 in the Department of Cardiology, Affiliated Hospital of Hebei University, were randomly divided into four groups: group 1 (immediate invasive strategy, percutaneous coronary interventions (PCI) < 24 hours after symptoms onset, n = 80), group 2 (early invasive strategy, 24-< 72 hours after symptoms onset, n = 80), group 3 (delayed invasive strategy after symptoms onset, 72-< 168 hours after symptoms onset, n = 80), and group 4 (late PCI group after symptoms onset, ≥ 168 hours after symptoms onset, n = 80). Primary study end points were 12-month cardiac mortality, nonfatal myocardial infarction (MI), target-vessel revascularization, and heart failure-related rehospitalization.
Results: There were no significant differences between groups in cardiac mortality, nonfatal MI and target-vessel revascularization. During follow-up, heart failure-related rehospitalization was higher in group 1 than in the other groups (18.8% vs. 5.1% vs. 7.4% vs. 6.3%, p = 0.010). Compared with group 1, group 2, group 3 and group 4 had lower heart failure-related rehospitalization (HR = 0.250, 95% CI: 0.083-0.753, p = 0.014) (HR = 0.377, 95% CI: 0.146-0.971, p = 0.043) (HR = 0.320, 95% CI: 0.116-0.879, p = 0.027).
Conclusions: For acute STEMI patients who missed the optimal time of PCI, immediate PCI did not reduce adverse clinical outcomes.
Keywords: acute ST segment elevated myocardial infarction; cardiac mortality; different timing of percutaneous coronary intervention; heart failure-related rehospitalization.
Copyright: © 2024 Polish Society of Cardiothoracic Surgeons (Polskie Towarzystwo KardioTorakochirurgów) and the editors of the Polish Journal of Cardio-Thoracic Surgery (Kardiochirurgia i Torakochirurgia Polska).
Conflict of interest statement
The authors report no conflict of interest.
Figures
References
-
- Bouisset F, Gerbaud E, Bataille V, Coste P, Puymirat E, Belle L, Delmas C, Cayla G, Motreff P, Lemesle G, Aissaoui N, Blanchard D, Schiele F, Simon T, Danchin N, Ferrières J; FAST-MI Investigators . Percutaneous myocardial revascularization in late-presenting patients with STEMI. J Am Coll Cardiol 2021; 78: 1291-1305. - PubMed
-
- Cohen M, Boiangiu C, Abidi M. Therapy for ST-segment elevation myocardial infarction patients who present late or are ineligible for reperfusion therapy. J Am Coll Cardiol 2010; 55: 1895-1906. - PubMed
-
- Lee PY, Alexander KP, Hammill BG, Pasquali SK, Peterson ED. Representation of elderly persons and women in published randomized trials of acute coronary syndromes. JAMA 2001; 286: 708-713. - PubMed
-
- Sacco A, Montalto C, Bravi F, Ruzzenenti G, Garatti L, Oreglia JA, Bartorelli AL, Crimi G, LA Vecchia C, Savonitto S, Leonardi S, Oliva FG, Morici N. Non-ST-elevation acute coronary syndrome in chronic kidney disease: prognostic implication of an early invasive strategy. Minerva Cardiol Angiol 2023; 71: 44-50. - PubMed
-
- Jobs A, Mehta SR, Montalescot G, Vicaut E, Van’t Hof AWJ, Badings EA, Neumann FJ, Kastrati A, Sciahbasi A, Reuter PG, Lapostolle F, Milosevic A, Stankovic G, Milasinovic D, Vonthein R, Desch S, Thiele H. Optimal timing of an invasive strategy in patients with non-ST-elevation acute coronary syndrome: a meta-analysis of randomised trials. Lancet 2017; 390: 737-746. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous