

This is a preprint.
Automated Deep Learning-Based Detection of Early Atherosclerotic Plaques in Carotid Ultrasound Imaging
- PMID: 39484270
- PMCID: PMC11527046
- DOI: 10.1101/2024.10.17.24315675
Automated Deep Learning-Based Detection of Early Atherosclerotic Plaques in Carotid Ultrasound Imaging
Abstract
Background: Carotid plaque presence is associated with cardiovascular risk, even among asymptomatic individuals. While deep learning has shown promise for carotid plaque phenotyping in patients with advanced atherosclerosis, its application in population-based settings of asymptomatic individuals remains unexplored.
Methods: We developed a YOLOv8-based model for plaque detection using carotid ultrasound images from 19,499 participants of the population-based UK Biobank (UKB) and fine-tuned it for external validation in the BiDirect study (N = 2,105). Cox regression was used to estimate the impact of plaque presence and count on major cardiovascular events. To explore the genetic architecture of carotid atherosclerosis, we conducted a genome-wide association study (GWAS) meta-analysis of the UKB and CHARGE cohorts. Mendelian randomization (MR) assessed the effect of genetic predisposition to vascular risk factors on carotid atherosclerosis.
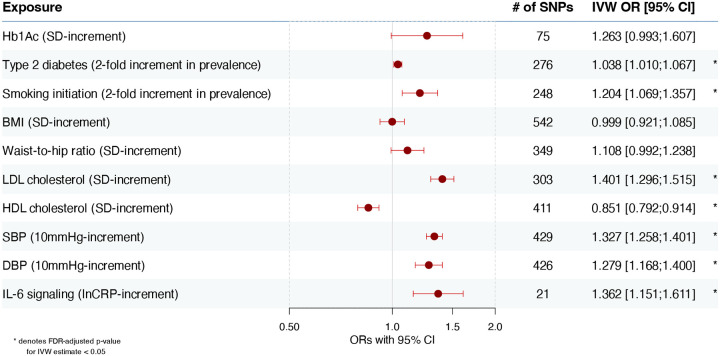
Results: Our model demonstrated high performance with accuracy, sensitivity, and specificity exceeding 85%, enabling identification of carotid plaques in 45% of the UKB population (aged 47-83 years). In the external BiDirect cohort, a fine-tuned model achieved 86% accuracy, 78% sensitivity, and 90% specificity. Plaque presence and count were associated with risk of major adverse cardiovascular events (MACE) over a follow-up of up to seven years, improving risk reclassification beyond the Pooled Cohort Equations. A GWAS meta-analysis of carotid plaques uncovered two novel genomic loci, with downstream analyses implicating targets of investigational drugs in advanced clinical development. Observational and MR analyses showed associations between smoking, LDL cholesterol, hypertension, and odds of carotid atherosclerosis.
Conclusions: Our model offers a scalable solution for early carotid plaque detection, potentially enabling automated screening in asymptomatic individuals and improving plaque phenotyping in population-based cohorts. This approach could advance large-scale atherosclerosis research.
Keywords: atherosclerosis; cardiovascular disease; carotid artery; genetics; machine learning; vascular ultrasound.
Figures





References
-
- Libby P, Buring JE, Badimon L, Hansson GK, Deanfield J, Bittencourt MS, Tokgözoğlu L, Lewis EF. Atherosclerosis. Nat. Rev. Dis. Primer. 2019;5:56.
-
- Naghavi M, Ong KL, Aali A, Ababneh HS, Abate YH, Abbafati C, Abbasgholizadeh R, Abbasian M, Abbasi-Kangevari M, Abbastabar H, et al. Global burden of 288 causes of death and life expectancy decomposition in 204 countries and territories and 811 subnational locations, 1990–2021: a systematic analysis for the Global Burden of Disease Study 2021. The Lancet. 2024;403:2100–2132.
-
- Ferrari AJ, Santomauro DF, Aali A, Abate YH, Abbafati C, Abbastabar H, Abd ElHafeez S, Abdelmasseh M, Abd-Elsalam S, Abdollahi A, et al. Global incidence, prevalence, years lived with disability (YLDs), disability-adjusted life-years (DALYs), and healthy life expectancy (HALE) for 371 diseases and injuries in 204 countries and territories and 811 subnational locations, 1990–2021: a systematic analysis for the Global Burden of Disease Study 2021. The Lancet. 2024;403:2133–2161.
-
- Joynt Maddox KE, Elkind MSV, Aparicio HJ, Commodore-Mensah Y, De Ferranti SD, Dowd WN, Hernandez AF, Khavjou O, Michos ED, Palaniappan L, et al. Forecasting the Burden of Cardiovascular Disease and Stroke in the United States Through 2050—Prevalence of Risk Factors and Disease: A Presidential Advisory From the American Heart Association. Circulation [Internet]. 2024. [cited 2024 Aug 19];150. Available from: https://www.ahajournals.org/doi/10.1161/CIR.0000000000001256 - DOI
-
- Goh RSJ, Chong B, Jayabaskaran J, Jauhari SM, Chan SP, Kueh MTW, Shankar K, Li H, Chin YH, Kong G, et al. The burden of cardiovascular disease in Asia from 2025 to 2050: a forecast analysis for East Asia, South Asia, South-East Asia, Central Asia, and high-income Asia Pacific regions. Lancet Reg. Health - West. Pac. 2024;49:101138. - PMC - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources