

Clinical parameters and postoperative outcomes of pituitary adenomas in children: Analysis according to size of adenomas and adopted surgical procedures
- PMID: 39484285
- PMCID: PMC11526202
- DOI: 10.3892/mco.2024.2792
Clinical parameters and postoperative outcomes of pituitary adenomas in children: Analysis according to size of adenomas and adopted surgical procedures
Abstract
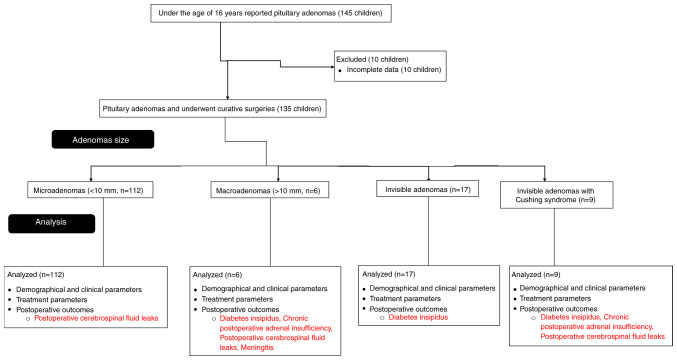
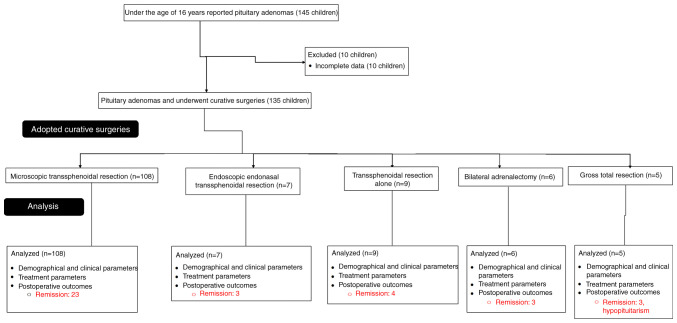
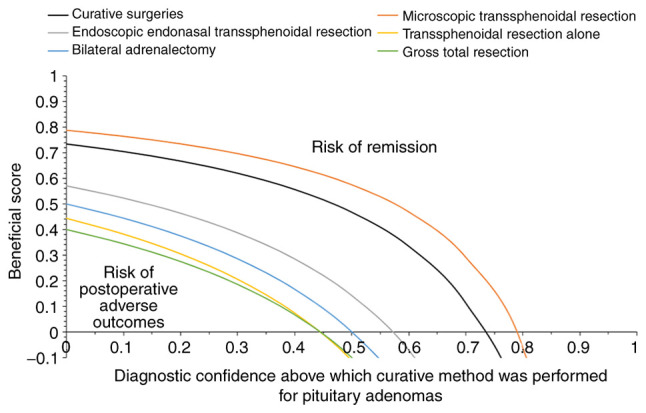
Pathologies of pediatric pituitary adenomas are uncommon and challenging to diagnose. Pituitary adenomas cause mass effects and neurological disruption in children. Postoperative evaluations of endocrine functions are challenging. The present study categorized adenomas by size and type, and evaluated outcomes based on the surgical procedures adopted. In addition, the present study analyzed the demographic parameters of children as well as the factors supposed to be influencing remission. Clinical characteristics, treatment parameters and postoperative outcomes of curative surgeries in 135 children [80 (59%) females and 55 (41%) males; age 12 (11-13) years at the time of first diagnosis] with pituitary adenomas who underwent curative surgeries operated between 1998 and 2023 in the Yichang Central People's Hospital, (Yichang, China) were included in the present retrospective study. A total of 112 (83%) children had microadenomas (<10 mm adenomas), 6 (4%) had macroadenomas (≥10 mm adenomas) and 17 (13%) had invisible adenomas. Pathological examination revealed that 59 (44%) children had functional adenomas and 10 (7%) had non-functional adenomas. Among functional adenomas, acromegaly (excess secretion of insulin-like growth factor 1) was reported to be the most common [30 (22%)] pediatric adenomas, followed by prolactinomas [prolactin secretion ≥1,000 mIU/l; 20 (15%) and Cushing syndrome (9 (7%)]. A total of 23 (17%), 3 (2%), 4 (3%), 3 (2%) and 3 (2%) children were reported to have remission and underwent re-surgery. These patients (remission) underwent microscopic trans-sphenoidal resection, endoscopic endonasal trans-sphenoidal resection, trans-sphenoidal resection alone, bilateral adrenalectomy and gross total resection adopted curative surgeries initially, respectively. Postoperative diabetes insipidus, adrenal insufficiency and cerebrospinal fluid leaks have been reported in children who have undergone curative surgeries for macroadenomas or Cushing syndrome. Female pediatric patients with clinical manifestations were more likely to have pituitary adenomas. Pediatric patients generally have functional pituitary adenomas, particularly adreno-corticotropin-secreting adenomas. Microscopic trans-sphenoidal resection is associated with a lower risk of under-treatment. Postoperative outcomes and clinical benefits of curative surgeries are based on the complete type of surgical removal and size of the pituitary adenomas mass (Level of Evidence: 3; Technical Efficacy Stage: 4).
Keywords: Cushing syndrome; acromegaly; functional adenomas; macroadenomas; microadenomas; microscopic trans-sphenoidal resection; pituitary adenoma; prolactinoma.
Copyright: © 2024 Li et al.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Impact of tumor characteristics and pre- and postoperative hormone levels on hormonal remission following endoscopic transsphenoidal surgery in patients with acromegaly.Neurosurg Focus. 2020 Jun;48(6):E10. doi: 10.3171/2020.3.FOCUS2080. Neurosurg Focus. 2020. PMID: 32480366
-
Diagnosis and treatment of pituitary adenomas.Minerva Endocrinol. 2004 Dec;29(4):241-75. Minerva Endocrinol. 2004. PMID: 15765032 Review.
-
Reoperative endoscopic endonasal surgery for residual or recurrent pituitary adenomas.J Neurosurg. 2017 Aug;127(2):397-408. doi: 10.3171/2016.8.JNS152709. Epub 2016 Oct 28. J Neurosurg. 2017. PMID: 27791524
-
Transsphenoidal surgery for pituitary adenomas in pediatric patients: a multicentric retrospective study.Childs Nerv Syst. 2019 Nov;35(11):2119-2126. doi: 10.1007/s00381-019-04179-z. Epub 2019 May 11. Childs Nerv Syst. 2019. PMID: 31079182
-
Reoperation for growth hormone-secreting pituitary adenomas: report on an endonasal endoscopic series with a systematic review and meta-analysis of the literature.J Neurosurg. 2018 Aug;129(2):404-416. doi: 10.3171/2017.2.JNS162673. Epub 2017 Sep 1. J Neurosurg. 2018. PMID: 28862548
Cited by
-
Radiological anatomy of sella turcica in children: a retrospective study with CT.Surg Radiol Anat. 2025 Apr 3;47(1):116. doi: 10.1007/s00276-025-03624-w. Surg Radiol Anat. 2025. PMID: 40180625
References
-
- Kelly AP, Greenfield JP, Dobri GA, Schwartz TH. Pediatric pituitary adenomas are more aggressive, more likely to be hormone producing and are more difficult to cure than adult pituitary adenomas: Case series and systematic literature review. Childs Nerv Syst. 2022;38:729–738. doi: 10.1007/s00381-022-05445-3. - DOI - PubMed
LinkOut - more resources
Full Text Sources