

Behavioral Interventions for Tobacco Cessation in Low- and Middle-Income Countries: A Systematic Review and Meta-analysis
- PMID: 39485008
- PMCID: PMC11931222
- DOI: 10.1093/ntr/ntae259
Behavioral Interventions for Tobacco Cessation in Low- and Middle-Income Countries: A Systematic Review and Meta-analysis
Abstract
Introduction: An estimated 78% of the total deaths attributable to smoking tobacco use occurred in low- and middle-income countries (LMICs) in 2019. In addition, smokeless tobacco increases the risk of all-cause mortality, all cancers, including upper aero-digestive tract cancer, stomach cancer, ischemic heart disease and stroke, with 88% of the mortality burden being borne by the South-East Asian region. Evidence-based interventions from high-income countries (HICs) are not easily transferable to LMICs, as patterns of tobacco use, health beliefs associated with tobacco use, and awareness of specific health risks vary substantially.
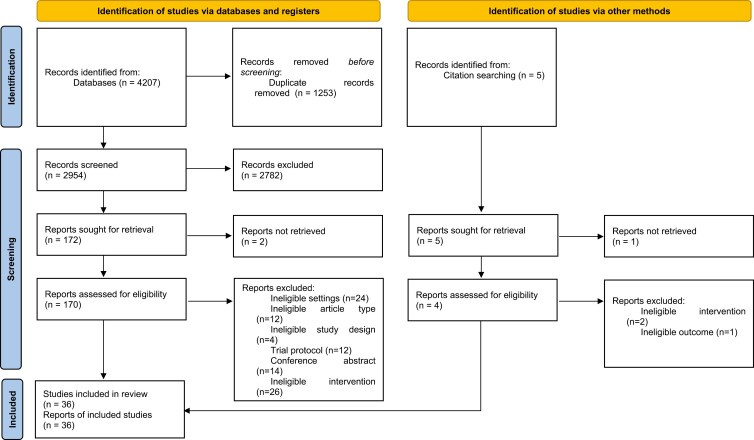
Methods: We synthesized the effectiveness of behavioral interventions for tobacco cessation in LMICs through a systematic review and meta-analysis. Interventional studies which delivered individual behavioral intervention and assessed abstinence from tobacco use were included. We examined the pooled intervention effect at 6 months postintervention follow-up.
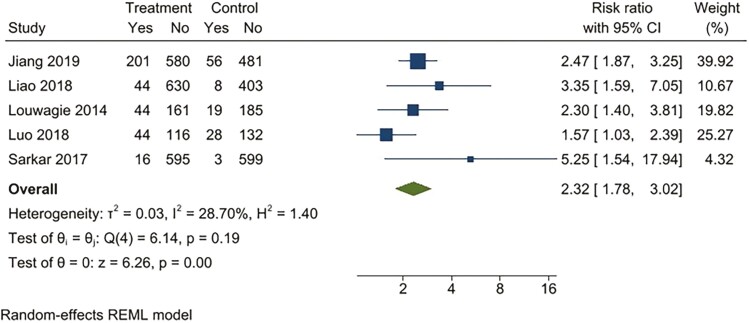
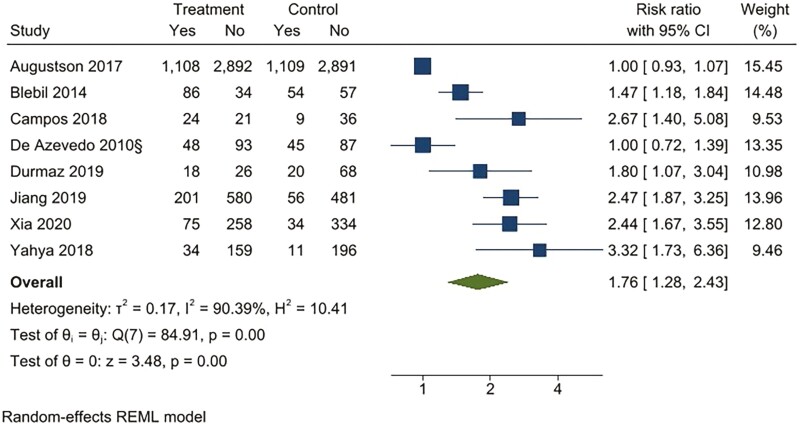
Results: For continuous abstinence at 6 months, the intervention was superior to the active comparator (RR 2.32; 95% CI 1.78 to 3.02) and usual care (RR 4.39; 95% CI 2.38 to 8.11). For point prevalence abstinence at six months, the intervention was superior to the active comparator (RR 1.76; 95% CI 1.28 to 2.44), and usual care (RR 2.37; 95% CI 1.47 to 3.81). The statistical heterogeneity was substantial to considerable for all comparisons. Only six studies had an overall low risk of bias. Publication bias was observed for all comparisons except for 6-month continuous outcomes.
Conclusions: Implementation research is needed to understand factors for programme sustainability and equity of the impact of behavioral interventions in reducing tobacco use in LMICs.
Implications: Our review is an important step towards understanding the effectiveness of behavior interventions for tobacco cessation suited for LMICs and which are responsive to the contextual needs of such countries.
© The Author(s) 2024. Published by Oxford University Press on behalf of the Society for Research on Nicotine and Tobacco.
Conflict of interest statement
None declared.
Figures



References
-
- Reitsma MB, Kendrick PJ, Ababneh E, et al. Spatial, temporal, and demographic patterns in prevalence of smoking tobacco use and attributable disease burden in 204 countries and territories, 1990–2019: a systematic analysis from the Global Burden of Disease Study 2019. Lancet. 2021;397(10292):2337–2360. - PMC - PubMed
-
- World Health Organization. WHO Global Report on Trends in Prevalence of Tobacco Use 2000–2025. Geneva: World Health Organization; 2021.
-
- Sinha DN, Suliankatchi RA, Gupta PC, et al. Global burden of all-cause and cause-specific mortality due to smokeless tobacco use: systematic review and meta-analysis. Tob Control. 2018;27(1):35–42. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
