

Cannabis Use During Early Pregnancy Following Recreational Cannabis Legalization
- PMID: 39485336
- PMCID: PMC11530934
- DOI: 10.1001/jamahealthforum.2024.3656
Cannabis Use During Early Pregnancy Following Recreational Cannabis Legalization
Abstract
Importance: It is unknown whether state recreational cannabis legalization (RCL) is related to increased rates of prenatal cannabis use or whether RCL-related changes vary with cannabis screening methods or the local policy environment.
Objective: To test whether RCL in California was associated with changes in prenatal cannabis use rates, whether changes were evident in both self-report and urine toxicology testing, and whether rates varied by local policies banning vs allowing adult-use retailers post-RCL.
Design, setting, and participants: This population-based time-series study used data from pregnancies in Kaiser Permanente Northern California universally screened for cannabis use during early pregnancy by self-report and toxicology testing from January 1, 2012, to December 31, 2019. Analyses were conducted from September 2022 to August 2024.
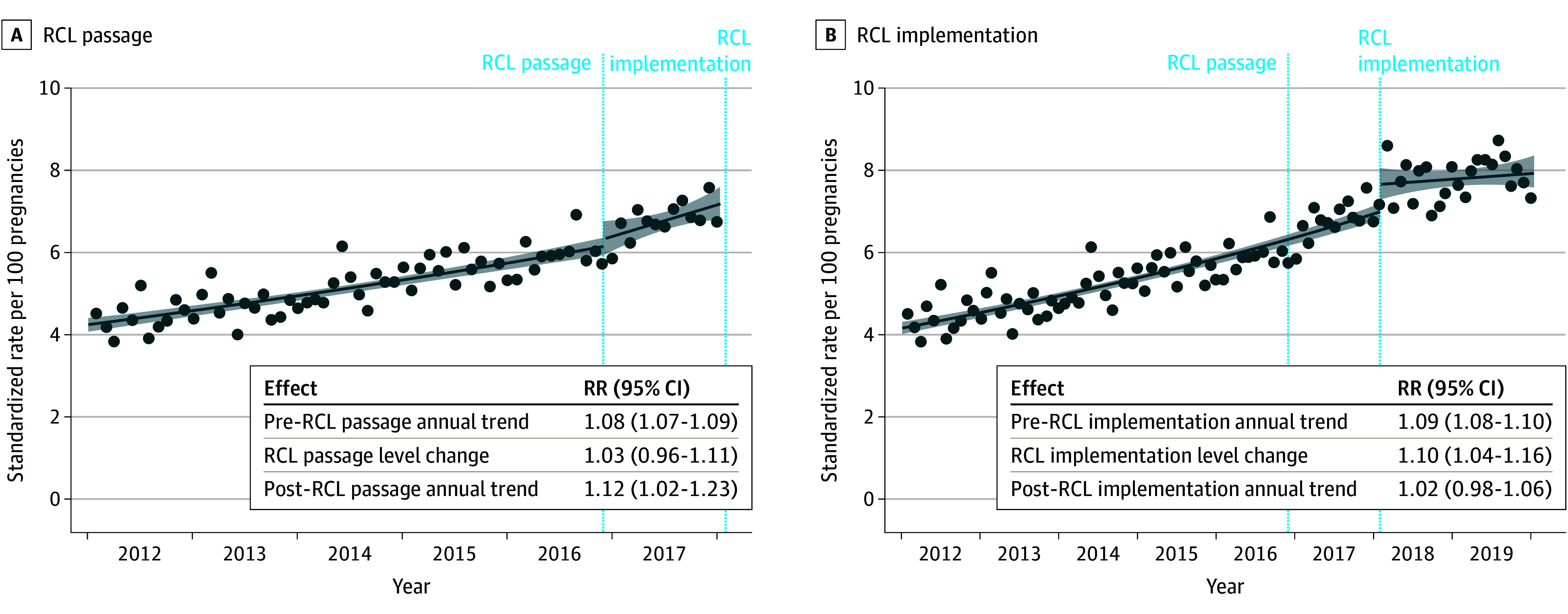
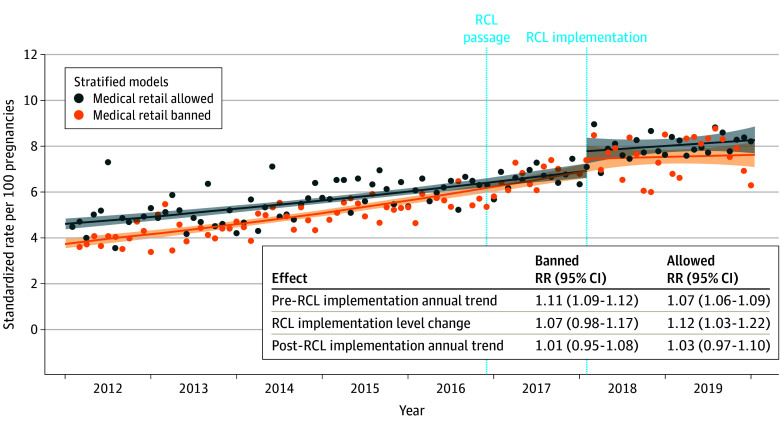
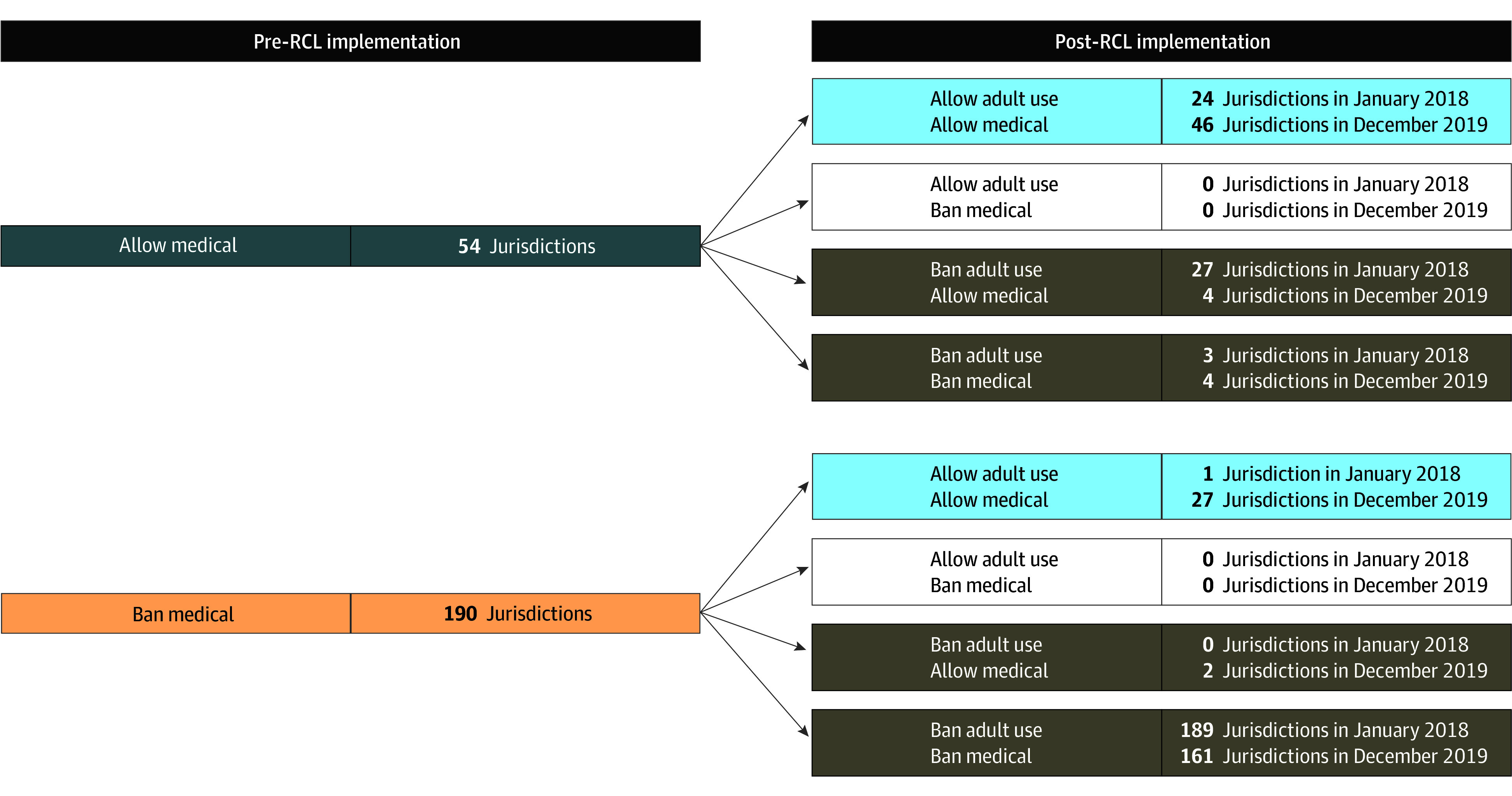
Exposures: California state RCL passage (November 9, 2016) and implementation of legal sales (January 1, 2018) were examined with a 1-month lag. Local policies allowing vs banning medical retailers pre-RCL and adult-use retailers post-RCL were also examined.
Main outcomes and measures: Any prenatal cannabis use was based on screening at entrance to prenatal care (typically at 8-10 weeks' gestation) and defined as (1) a positive urine toxicology test result or self-report, (2) a positive urine toxicology test result, or (3) self-report. Interrupted time series models were fit using Poisson regression, adjusting for age, race and ethnicity, and neighborhood deprivation index.
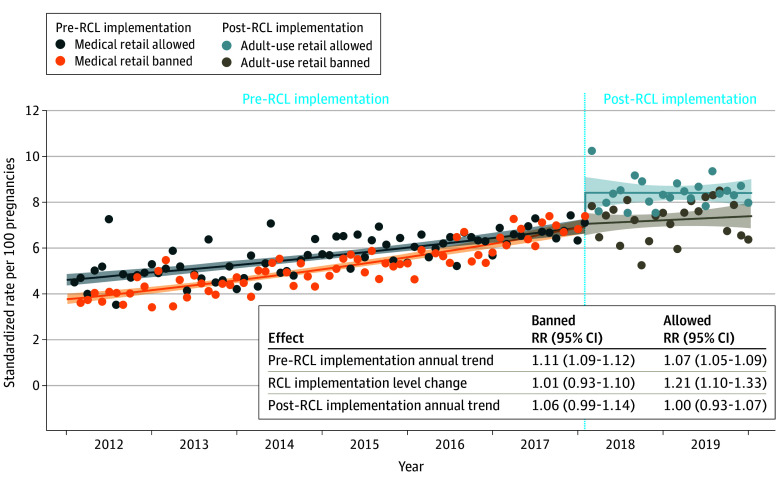
Results: The sample of 300 993 pregnancies (236 327 unique individuals) comprised 25.9% Asian individuals, 6.4% Black individuals, 26.0% Hispanic individuals, 37.7% White individuals, and 4.1% individuals of other, multiple, or unknown race, with a mean (SD) age of 30.3 (5.4) years. Before RCL implementation, rates of prenatal cannabis use rose steadily from 4.5% in January 2012 to 7.1% in January 2018. There was no change in use rates at the time of RCL passage (level change rate ratio [RR], 1.03; 95% CI, 0.96-1.11) and a statistically significant increase in rates in the first month after RCL implementation, increasing to 8.6% in February 2018 (level change RR, 1.10; 95% CI, 1.04-1.16). Results were similar when defining prenatal cannabis use by (1) a toxicology test or (2) self-report. In local policy analyses, the post-RCL implementation increase in use was only found among those in jurisdictions allowing adult-use cannabis retailers (allowed RR, 1.21; 95% CI, 1.10-1.33; banned RR, 1.01; 95% CI, 0.93-1.10).
Conclusions and relevance: In this time-series study, RCL implementation in California was associated with an increase in rates of cannabis use during early pregnancy, defined by both self-report and toxicology testing, driven by individuals living in jurisdictions that allowed adult-use retailers.
Conflict of interest statement
Figures
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
