

Anemia Acuity Effect on Transfusion Strategies in Acute Myocardial Infarction: A Secondary Analysis of the MINT Trial
- PMID: 39485351
- PMCID: PMC11530937
- DOI: 10.1001/jamanetworkopen.2024.42361
Anemia Acuity Effect on Transfusion Strategies in Acute Myocardial Infarction: A Secondary Analysis of the MINT Trial
Abstract
Importance: In patients with acute myocardial infarction (MI), limited physiologic adaptation to acute anemia might lead to greater benefit from a liberal red blood cell (RBC) transfusion strategy. Data on such a possible benefit are lacking.
Objectives: To compare acute anemia with chronic anemia and post-MI outcomes and estimate the differential effect of a restrictive RBC transfusion strategy compared with a liberal strategy on post-MI outcomes according to anemia acuity.
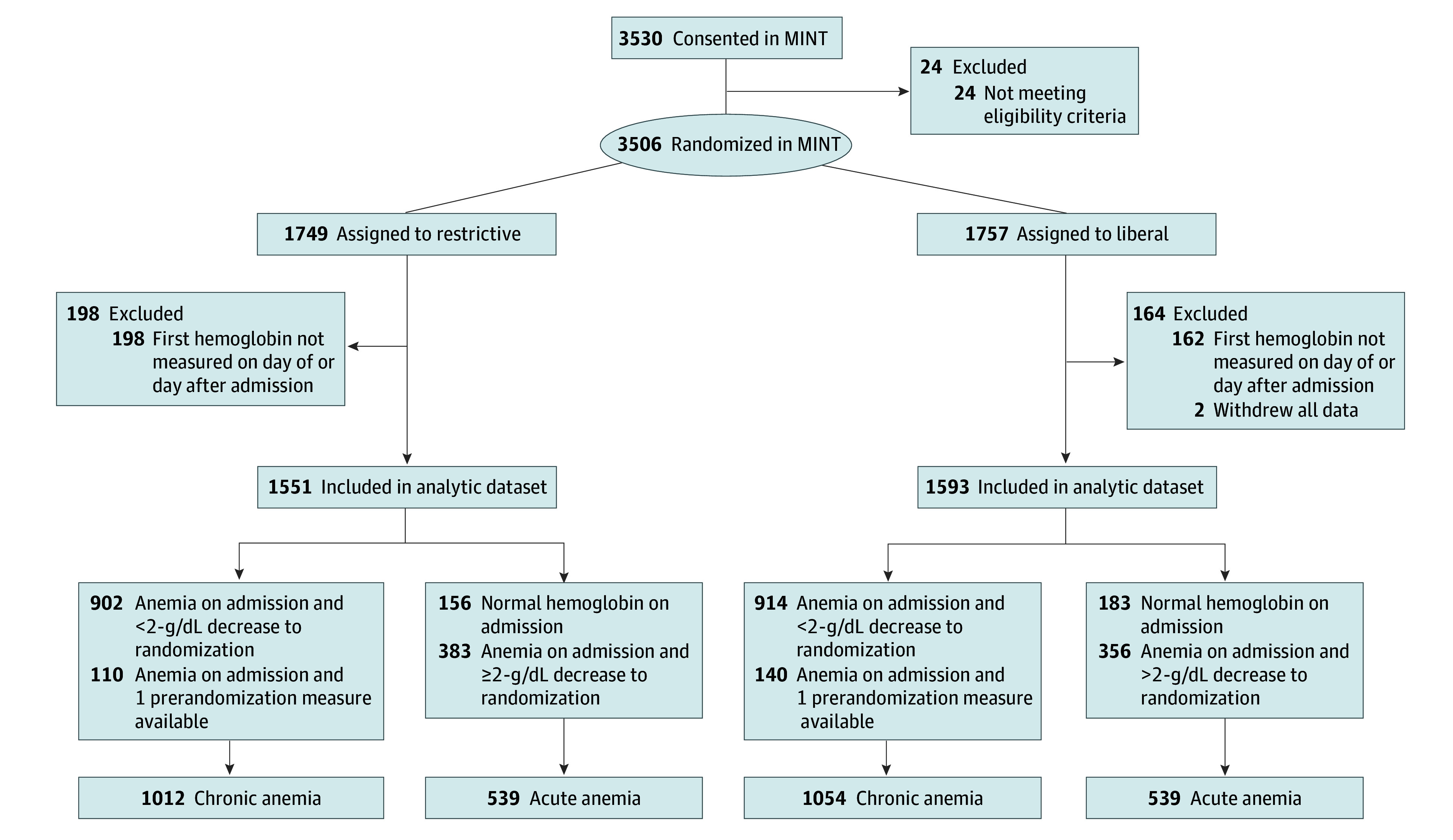
Design, setting, and participants: A prespecified subgroup analysis of the Myocardial Ischemia and Transfusion (MINT) multicenter randomized clinical trial was conducted in 126 hospitals in 6 countries between April 26, 2017, and April 14, 2023, with 30-day follow-up and blinded adjudication of the primary outcome. The analysis included 3144 of 3504 MINT participants (89.7%) with acute MI, a hemoglobin (Hb) level less than 10 g/dL at randomization, and a first Hb measurement available on the day of or the day following hospital admission.
Intervention: The MINT trial randomized participants to a restrictive (Hb <7-8 g/dL) or liberal (Hb <10 g/dL) RBC transfusion strategy. Acute anemia was defined as having a first Hb value greater than 13 g/dL (men) or 12 g/dL (women), or as having a decrease greater than or equal to 2 g/dL between the first Hb measurement and measurement at randomization. Other Hb levels were categorized as chronic anemia.
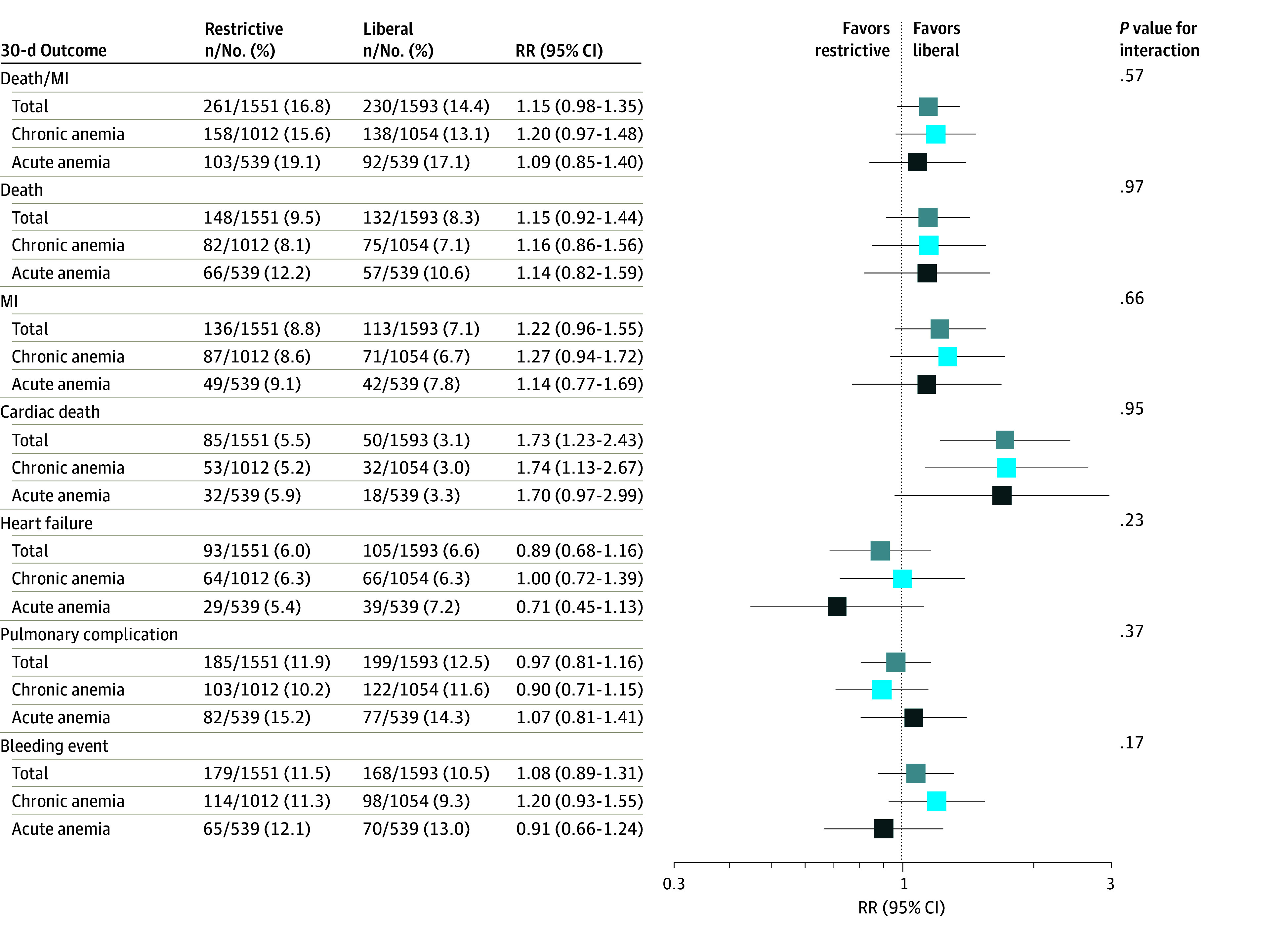
Main outcomes and measures: The primary outcome was a composite of death or recurrent MI up to 30 days after randomization. Secondary outcomes were death, recurrent MI, cardiac death, heart failure, pulmonary complications, and major bleeding events. Intention-to-treat analysis was performed.
Results: Among 3144 included participants (mean [SD] age, 72.3 [11.6] years; 1715 [54.5%] male; 1307 [41.6%] with type 1 MI), 1078 [34.3%]) had acute anemia. Acute anemia was associated with an increased risk of death or recurrent MI (adjusted risk ratio, 1.25; 95% CI, 1.05-1.48). The effect of a restrictive RBC transfusion strategy compared with a liberal strategy was similar for participants with either acute or chronic anemia for all outcomes.
Conclusions and relevance: In this secondary analysis of the MINT trial, acute anemia was associated with less favorable post-MI outcomes than chronic anemia but did not modify the effects of the randomized transfusion strategy. In patients with anemia and MI, the acuity of anemia should not influence the choice of transfusion trigger.
Trial registration: ClinicalTrials.gov Identifier: NCT02981407.
Conflict of interest statement
Figures
References
-
- Kunadian V, Mehran R, Lincoff AM, et al. . Effect of anemia on frequency of short- and long-term clinical events in acute coronary syndromes (from the Acute Catheterization and Urgent Intervention Triage Strategy Trial). Am J Cardiol. 2014;114(12):1823-1829. doi:10.1016/j.amjcard.2014.09.023 - DOI - PubMed
-
- Tsujita K, Nikolsky E, Lansky AJ, et al. . Impact of anemia on clinical outcomes of patients with ST-segment elevation myocardial infarction in relation to gender and adjunctive antithrombotic therapy (from the HORIZONS-AMI trial). Am J Cardiol. 2010;105(10):1385-1394. doi:10.1016/j.amjcard.2010.01.001 - DOI - PubMed
-
- Mamas MA, Kwok CS, Kontopantelis E, et al. . Relationship between anemia and mortality outcomes in a national acute coronary syndrome cohort: insights from the UK Myocardial Ischemia National Audit Project Registry. J Am Heart Assoc. 2016;5(11):e003348. doi:10.1161/JAHA.116.003348 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
