

Meal Timing and Anthropometric and Metabolic Outcomes: A Systematic Review and Meta-Analysis
- PMID: 39485353
- PMCID: PMC11530941
- DOI: 10.1001/jamanetworkopen.2024.42163
Meal Timing and Anthropometric and Metabolic Outcomes: A Systematic Review and Meta-Analysis
Abstract
Importance: Meal timing strategies, such as time-restricted eating (TRE), reducing meal frequency, or altering calorie distribution across the day, have gained interest for their potential to enhance weight loss and metabolic health, particularly in managing chronic diseases, yet their long-term benefits are not known.
Objective: To evaluate the association between meal timing strategies (≥12 weeks) and anthropometric and metabolic indicators.
Data sources: Medline, Embase, CINAHL, and Cochrane CENTRAL were searched from inception to October 17, 2023.
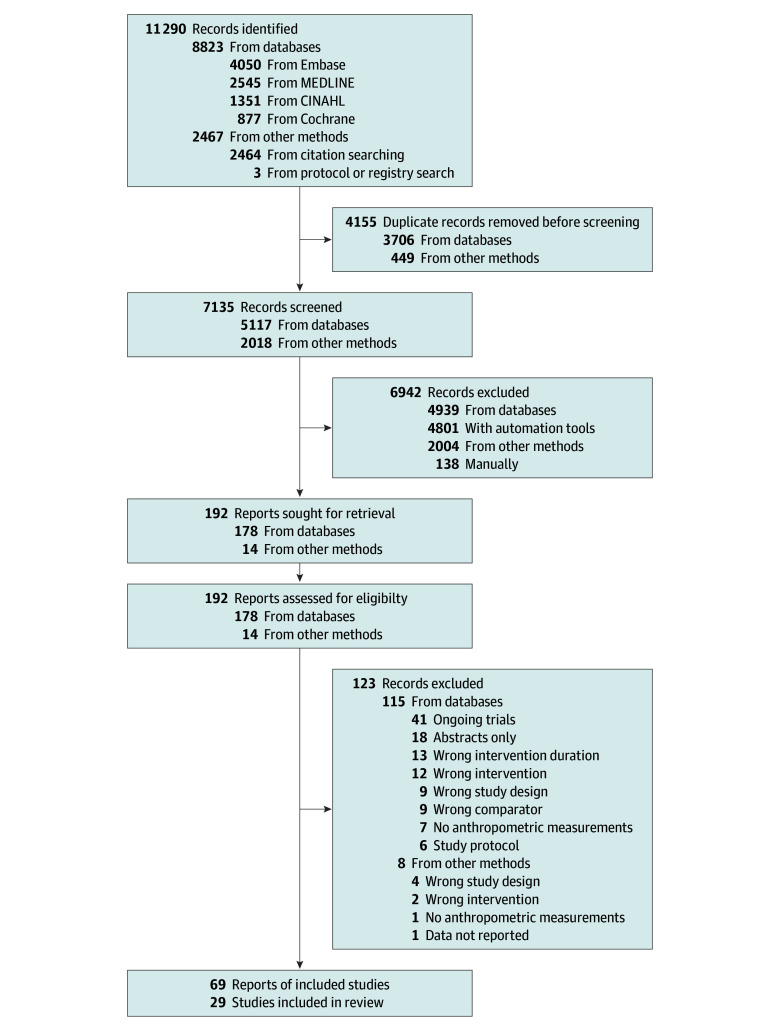
Study selection: Randomized clinical trials, regardless of language and publication date, involving adults 18 years and older, evaluating within-day meal timing patterns for 12 or more weeks, and reporting anthropometric measures were included. Studies were excluded if participants had eating disorders, prior significant weight change, underwent bariatric surgery, were pregnant, or if controlled variables differed between groups.
Data extraction and synthesis: Study quality was determined via Risk of Bias 2.0 tool. Data were extracted independently by multiple reviewers. Preferred Reporting Items for Systematic Reviews and Meta-analyses guidelines were used. Meta-analysis was performed using random-effects model on pooled continuous outcomes with 2 or more studies.
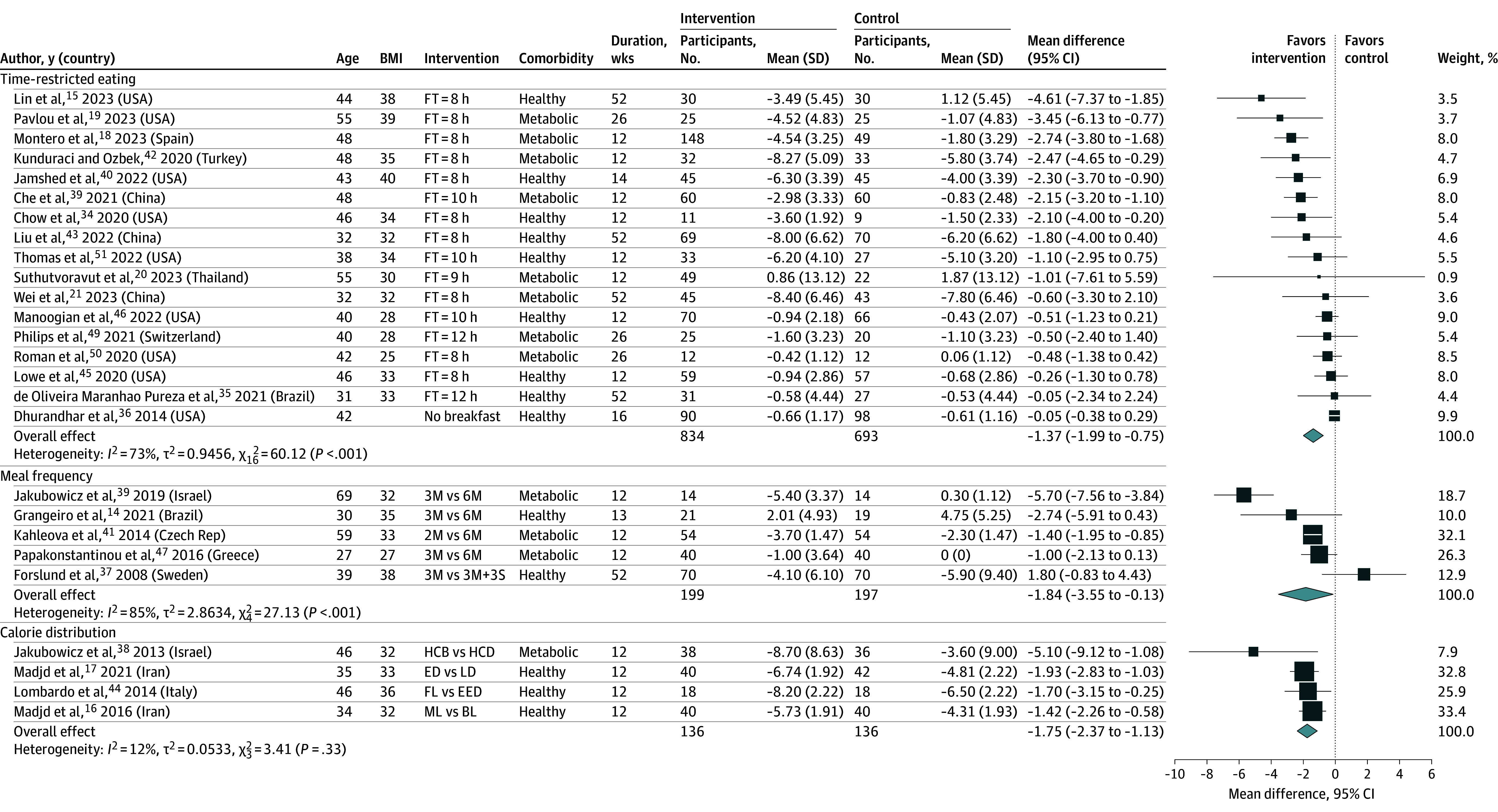
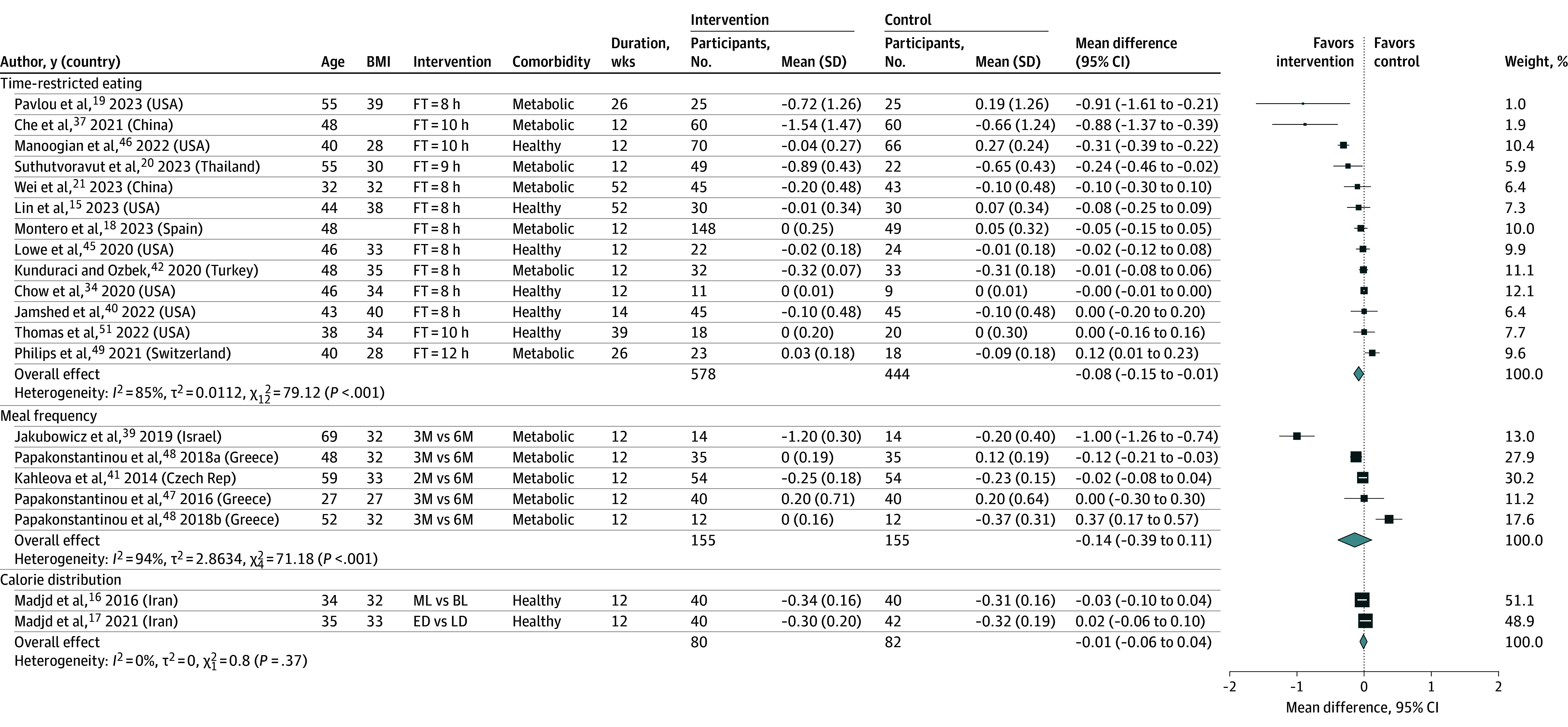
Main outcome and measures: Weight change in kilograms, reported as between-group mean difference with 95% CIs.
Results: Sixty-nine reports of 29 randomized clinical trials including 2485 individuals (1703 [69%] female; mean [SD] age, 44 [9.5] years; and mean [SD] body mass index, 33 [3.5]) were included. Study interventions included TRE (17 studies), meal frequency (8 studies), and calorie distribution (4 studies). There were some concerns of risk of bias for 7 studies and high concerns for 22 studies. Statistically significant weight change was observed in TRE when compared with control (-1.37 kg; 95% CI, -1.99 to -0.75 kg). Lower meal frequency and earlier caloric distribution were also both associated with greater change (-1.85 kg; 95% CI, -3.55 to -0.13 kg; and -1.75 kg; 95% CI, -2.37 to -1.13 kg, respectively).
Conclusions and relevance: The findings of this meta-analysis suggest that TRE, lower meal frequency, and earlier caloric distribution in the day may reduce weight compared with standard care and/or nutritional advice; however, the effect sizes found were small and of uncertain clinical importance. High heterogeneity and risk of bias among included studies led to concerns about the certainty of the underpinning evidence. Further research, including trials with larger sample sizes, standardized interventions with prescribed or matched energy intake, and longer follow-up, are needed.
Conflict of interest statement
Figures
Comment in
References
-
- World Health Organisation . Obesity and overweight. Updated March 1, 2024. Accessed March 14, 2024. https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight
-
- Di Angelantonio E, Bhupathiraju ShN, Wormser D, et al. ; Global BMI Mortality Collaboration . Body-mass index and all-cause mortality: individual-participant-data meta-analysis of 239 prospective studies in four continents. Lancet. 2016;388(10046):776-786. doi: 10.1016/S0140-6736(16)30175-1 - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
