

Changes in portal pulsatility index induced by a fluid challenge in patients with haemodynamic instability and systemic venous congestion: a prospective cohort study
- PMID: 39485575
- PMCID: PMC11530414
- DOI: 10.1186/s13613-024-01391-2
Changes in portal pulsatility index induced by a fluid challenge in patients with haemodynamic instability and systemic venous congestion: a prospective cohort study
Abstract
Background: It is uncertain whether fluid administration can improve patients with systemic venous congestion and haemodynamic instability. This study aimed to describe the changes in systemic venous congestion and peripheral perfusion parameters induced by a fluid challenge in these patients, and to analyse the influence of the fluid responsiveness status on these changes.
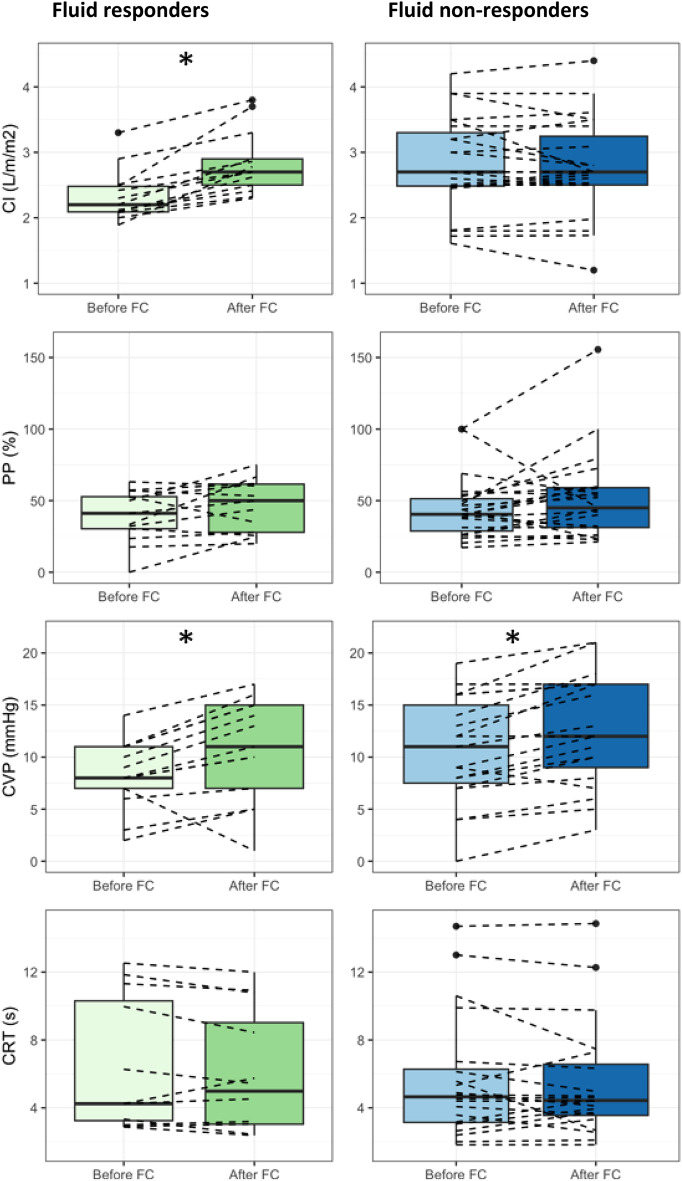
Methods: The study is a single-centre prospective cohort study of 36 critically ill ICU patients with haemodynamic instability and a maximum vena cava diameter ≥ 20 mm. Changes in cardiac index during a fluid challenge (4 mL/kg of lactated Ringer's solution during 5 min) assessed by pulse contour analysis, central venous pressure, ultrasound systemic congestion parameters (portal venous flow pulsatility index, supra hepatic and intrarenal venous Doppler), and peripheral perfusion parameters (capillary refill time and peripheral perfusion index) were assessed in the overall population. All these data were compared between patients presenting a cardiac index increase > 10% during the fluid challenge (fluid responders) and the others (fluid non-responders).
Results: Twenty-eight (78%) patients were admitted for postoperative care following cardiac surgery; their mean ± SD left ventricular ejection fraction was 42 ± 9% and right ventricular dysfunction was found in at least 61% of the patients. The mean ± SD SOFA score was 9 ± 3. Thirteen (36%) patients were fluid responders. The fluid challenge administration induced a significant increase in portal pulsatility index, VExUS score, and central venous pressure without significant difference of these changes between fluid responders and non-responders. No significant change in perfusion parameters was observed.
Conclusion: Fluid administration in patients with haemodynamic instability and systemic venous congestion worsens venous congestion regardless of the fluid responsiveness status, without improving perfusion parameters.
Keywords: Haemodynamic instability; Portal pulsatility index; Preload responsiveness; Systemic venous congestion; Ultrasound.
© 2024. The Author(s).
Conflict of interest statement
The authors have no conflicts of interest related to the study to declare.
Figures
References
LinkOut - more resources
Full Text Sources
