

Mesh-associated pain syndrome: predictors for continence and prolapse mesh removal surgery in a single centre
- PMID: 39487432
- PMCID: PMC11529248
- DOI: 10.1186/s12905-024-03393-5
Mesh-associated pain syndrome: predictors for continence and prolapse mesh removal surgery in a single centre
Abstract
Objective: Over the last two decades one of the main surgical treatment for stress urinary incontinence (SUI) and pelvic organ prolapse (POP) surgery was the insertion of non-absorbable mesh to restore continence and prolapse respectively. Over time complications arose including mesh-associated pain syndrome (MAPS), mesh exposure, mesh, erosion, chronic bladder/vaginal infections, and dyspareunia. Consequently, women chose surgical mesh removal to counter these problems. However, little is known about the demographics, medical co-morbidities, mesh types involved and the timing from mesh insertion to mesh removal. This retrospective study will look at which of these factors may be closely associated with mesh removal surgery.
Design: Retrospective evaluation.
Setting: Female Pelvic Medicine and Reconstructive Surgery (FPMRS) Clinic at University College London Hospitals NHS Foundation Trust.
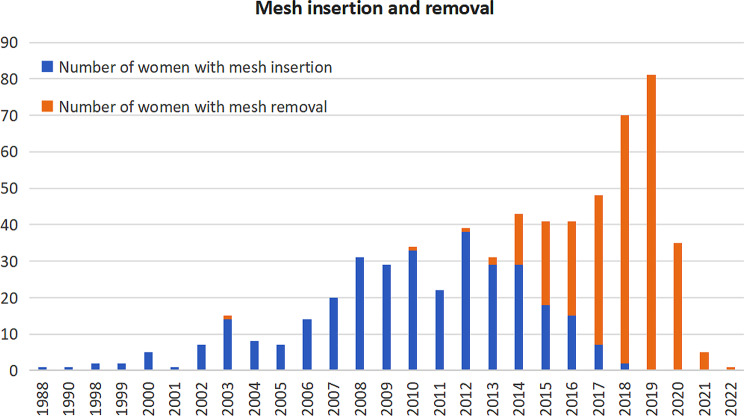
Population: All patients presenting to the FPMRS Clinic between June 2011 to December 2019, requesting mesh removal surgery with a history of MAPS and other mesh complications were included in this study.
Methods: Patient demographics including age, ethnicity, obstetric history, and medical co-morbidities; type of mesh/anatomical route used; onset of symptoms; and time from insertion to removal were recorded.
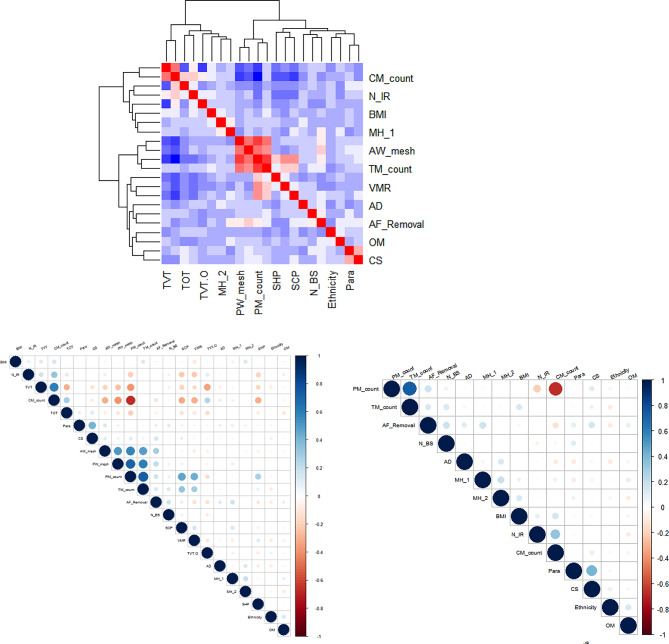
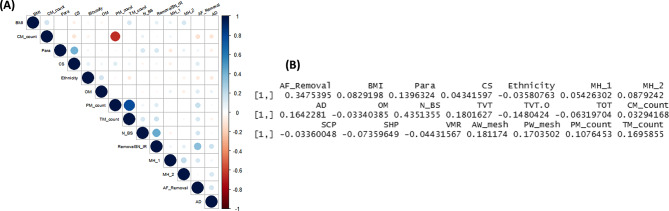
Main outcome measures: Determination of correlation coefficients between patient demographics, patient reported symptoms and mesh removal surgery.
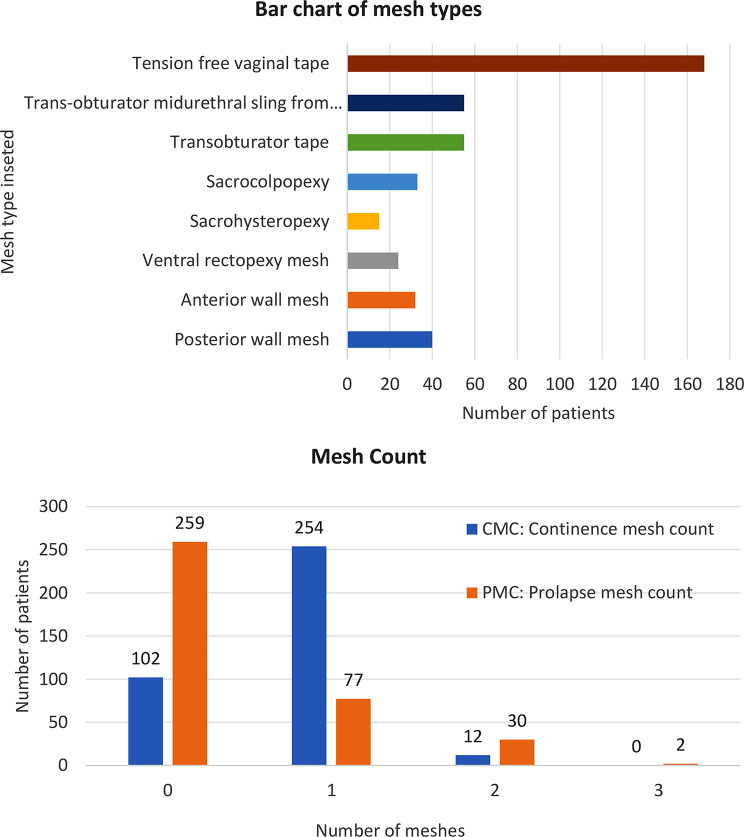
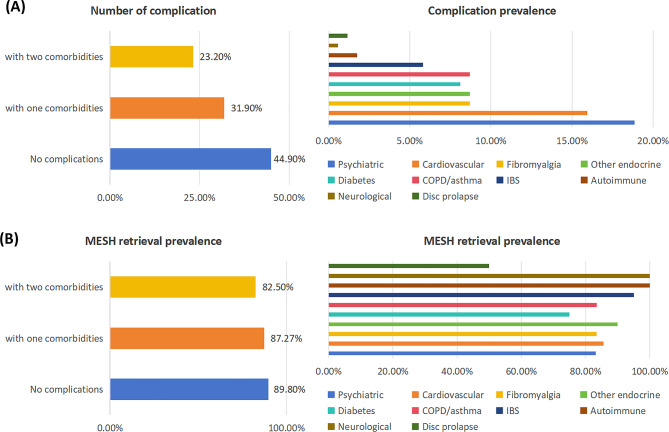
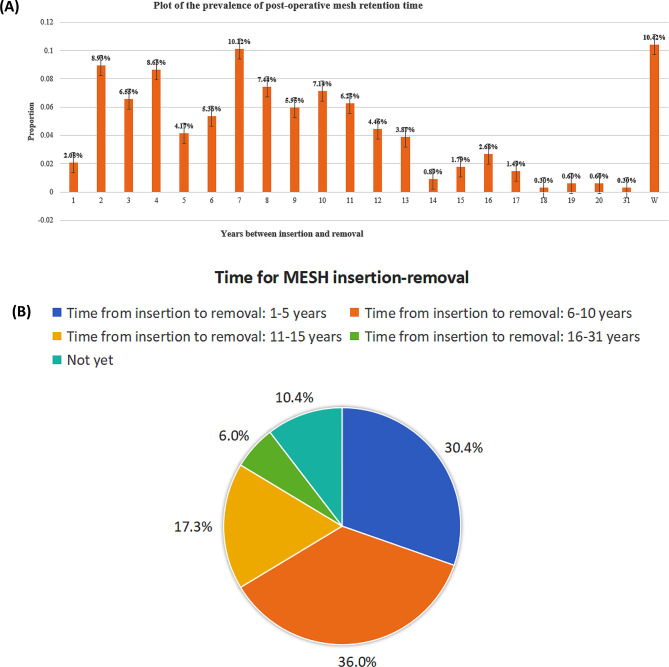
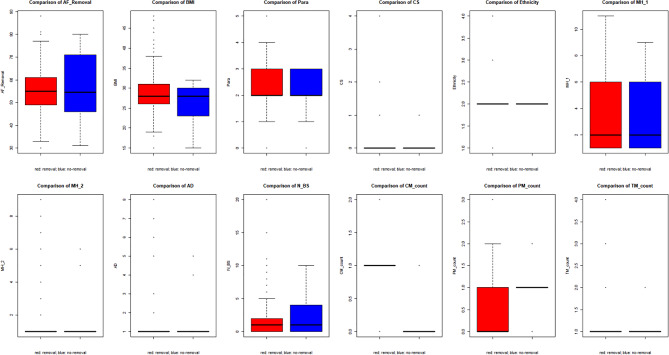
Results: Three hundred and forty-five women with a history of MAPS were included in the study. Women in the 40-60 year old cohort accounted for 54.4% of mesh removal surgery; 54.8% had a BMI under 30 and almost 90% were Caucasian. 96.5% had had children, with over 77% having had a vaginal delivery. 91.9% of patients reported other health conditions including 18.8% with a concomitant history of mental health problems and 15.4% with a history of heart disease. Over 80% of women undergoing mesh removal surgery had a continence mesh (49% retropubic and 32% obturator continence mesh) removed, whereas 20% had an abdominal prolapse and/or vaginal prolapse mesh removed. The average time from mesh insertion to mesh removal was seven years, with the prevalence of mesh removal surgery averaging 85% (range 50-100%) depending on the comorbidity determined.
Conclusions: All women presented to the clinic with a history of MAPS and other comorbidities which may have influenced their decision to pursue mesh removal surgery. There were no specific predictors, other than chronic pain associated with mesh, determining which women underwent surgery, though those with continence mesh were more likely to do so.
Keywords: Comorbidity; Continence mesh; Prolapse mesh; Surgery.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Slack M, Mayne C. Scientific Impact Paper No. 19: the use of mesh in gynaecological surgery, in Scientific Impact Paper. Royal College of Obstetricians and Gynaecologists; 2010.
-
- Amid PK. Classification of biomaterials and their related complications in abdominal wall hernia surgery. Hernia. 1997;1(1):15–21. - DOI
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
