

Distinct comorbidity phenotypes among post-9/11 Veterans with epilepsy are linked to diverging outcomes and mortality risks
- PMID: 39487827
- PMCID: PMC11742646
- DOI: 10.1111/epi.18170
Distinct comorbidity phenotypes among post-9/11 Veterans with epilepsy are linked to diverging outcomes and mortality risks
Abstract
Objective: To investigate phenotypes of comorbidity before and after an epilepsy diagnosis in a national cohort of post-9/11 Service Members and Veterans and explore phenotypic associations with mortality.
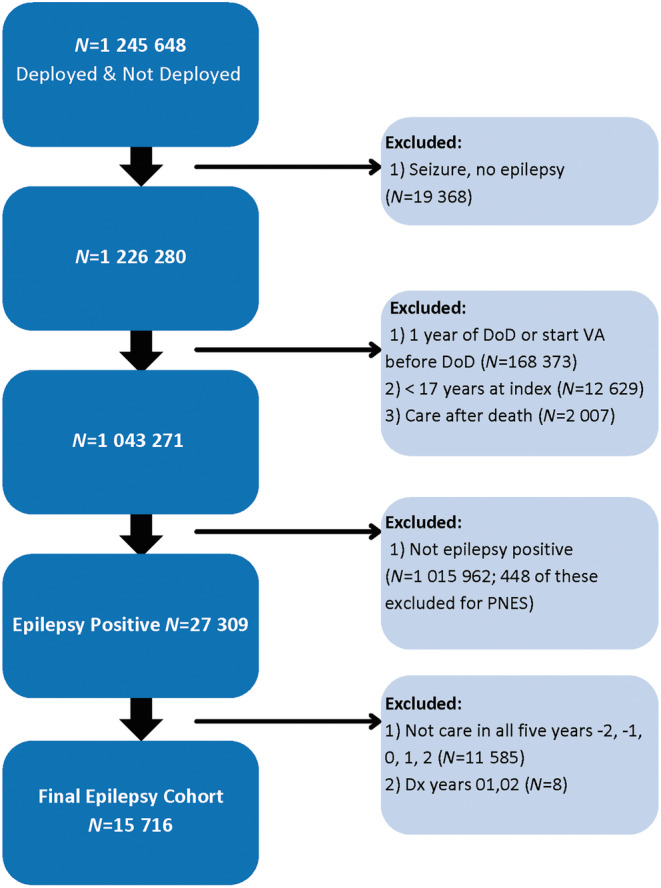
Methods: Among a longitudinal cohort of Service Members and Veterans receiving care in the Veterans Health Administration (VHA) from 2002 to 2018, annual diagnoses for 26 conditions associated with epilepsy were collected over 5 years, ranging from 2 years prior to 2 years after the year of first epilepsy diagnosis. Latent class analysis (LCA) was used to identify probabilistic comorbidity phenotypes with distinct health trajectories. Descriptive statistics were used to describe the characteristics of each phenotype. Fine and Gray cause-specific survival models were used to measure mortality outcomes for each phenotype up to 2021.
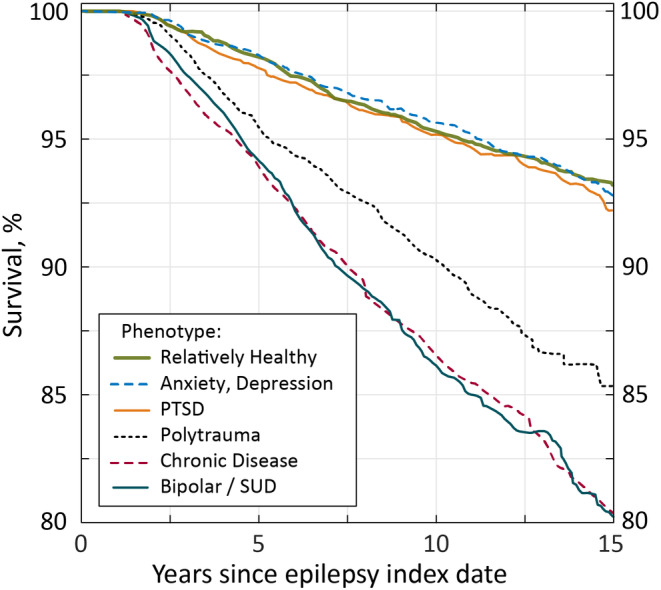
Results: Six distinct phenotypes were identified: (1) relatively healthy, (2) post-traumatic stress disorder, (3) anxiety and depression, (4) chronic disease, (5) bipolar/substance use disorder, and (6) polytrauma. Accidents were the most common cause of death overall, followed by suicide/mental health and cancer, respectively. Each phenotype exhibited unique associations with mortality and cause of death, highlighting the differential impact of comorbidity patterns on patient outcomes.
Significance: By delineating clinically meaningful epilepsy comorbidity phenotypes, this study offers a framework for clinicians to tailor interventions. Moreover, these data support systems of care that facilitate treatment of epilepsy and comorbidities within an interdisciplinary health team that allows continuity of care. Targeting treatment toward patients with epilepsy who present with specific heightened risks could help mitigate adverse outcomes and enhance overall patient care.
Keywords: epilepsy; mental health; phenotype; somatic comorbidity; traumatic brain injury.
Published 2024. This article is a U.S. Government work and is in the public domain in the USA. Epilepsia published by Wiley Periodicals LLC on behalf of International League Against Epilepsy.
Conflict of interest statement
We confirm that we have read the Journal's position on issues involved in ethical publication and affirm that this report is consistent with those guidelines. M.J. Pugh's institutions receive and has received (in the past 5 years) research grant funding from the National Institutes of Health, Department of Defense, and the Department of Veterans Affairs, and is employed by the Department of Veterans Affairs and the University of Utah. Dr. Pugh also received funding from Sanofi unrelated to epilepsy research. H. Munger Clary reports research funding from the National Institutes of Health, Department of Defense, National Science Foundation, Duke Endowment, Susanne Marcus Collins Foundation, and Eysz, Inc. E. Kennedy reports research funded by the Department of Defense.
S. Hinds reports consultant for SCS Consulting, LLC. Dr. Hinds has also received funding from the Department of Defense and National Institutes of Health and was previously employed by the Department of Defense. W. LaFrance reports research funded by the Department of Defense. H. Altalib reports that his institution has received research support from UCB, Eisai, and Sunovian. The institution of Dr. Altalib has received research support from the Department Of Defense—Congressionally Directed Medical Research Programs. A. Towne reports research grants from CURE and AbbVie (unrelated to epilepsy research) and participation on speakers' bureaus for AbbVie. Dr. Towne has also received funding from the Department of Defense and Department of Veterans Affairs, and is employed by the Department of Veterans Affairs and Virginia Commonwealth University. The remaining authors have no conflicts of interest to disclose.
Figures


References
-
- Lolk K, Lange T, Elwert F, Dreier JW, Christensen J. Traumatic brain injury, stroke, and epilepsy: a mediation study in a Danish nationwide cohort. Epilepsia. 2023;64:718–727. - PubMed
-
- Pugh MJ, Orman JA, Jaramillo CA, Salinsky MC, Eapen BC, Towne AR, et al. The prevalence of epilepsy and association with traumatic brain injury in veterans of the Afghanistan and Iraq wars. J Head Trauma Rehabil. 2015;30:29–37. - PubMed
-
- Ritter AC, Wagner AK, Fabio A, Pugh MJ, Walker WC, Szaflarski JP, et al. Incidence and risk factors of posttraumatic seizures following traumatic brain injury: a traumatic brain injury model systems study. Epilepsia. 2016;57:1968–1977. - PubMed
-
- Mahler B, Carlsson S, Andersson T, Tomson T. Risk for injuries and accidents in epilepsy: a prospective population‐based cohort study. Neurology. 2018;27(90):e779–e789. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
