

Efficacy of xanomeline and trospium chloride in schizophrenia: pooled results from three 5-week, randomized, double-blind, placebo-controlled, EMERGENT trials
- PMID: 39488504
- PMCID: PMC11531488
- DOI: 10.1038/s41537-024-00525-6
Efficacy of xanomeline and trospium chloride in schizophrenia: pooled results from three 5-week, randomized, double-blind, placebo-controlled, EMERGENT trials
Erratum in
-
Author Correction: Efficacy of xanomeline and trospium chloride in schizophrenia: pooled results from three 5-week, randomized, double-blind, placebo-controlled, EMERGENT trials.Schizophrenia (Heidelb). 2025 Mar 18;11(1):44. doi: 10.1038/s41537-025-00595-0. Schizophrenia (Heidelb). 2025. PMID: 40102406 Free PMC article. No abstract available.
Abstract
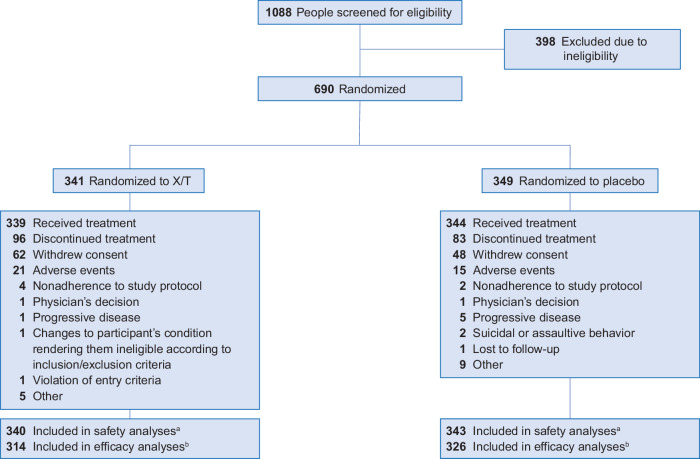
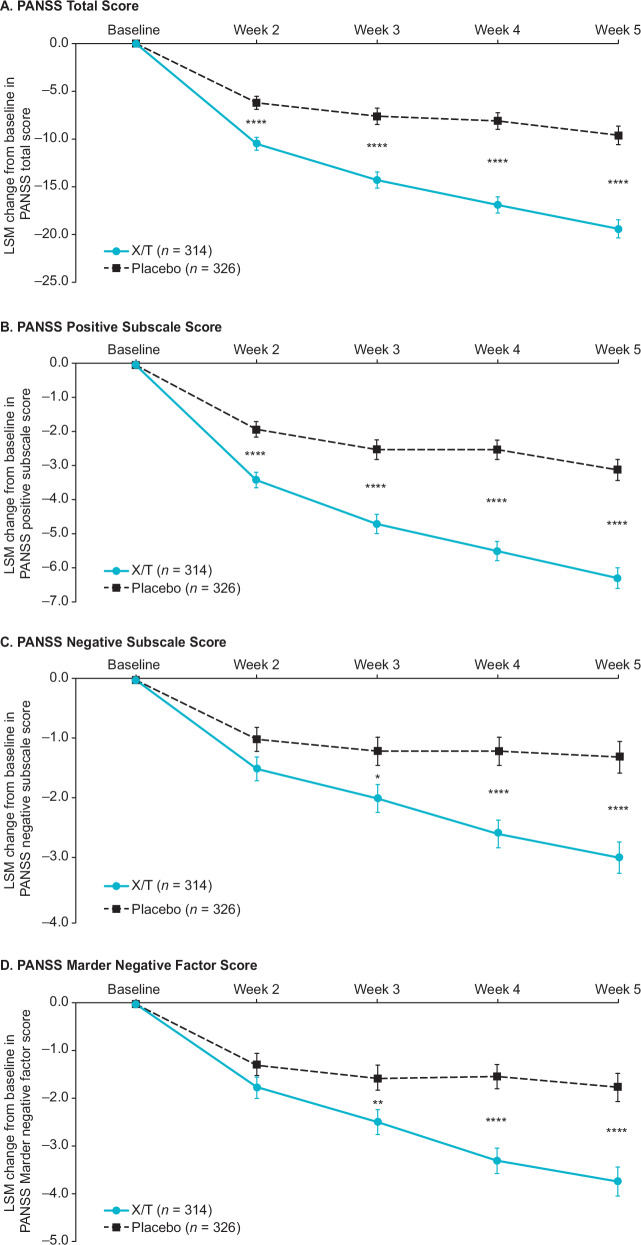
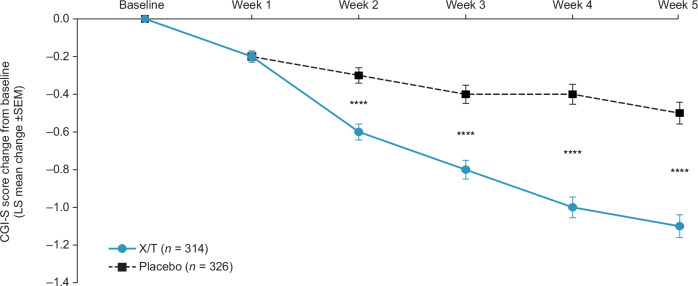
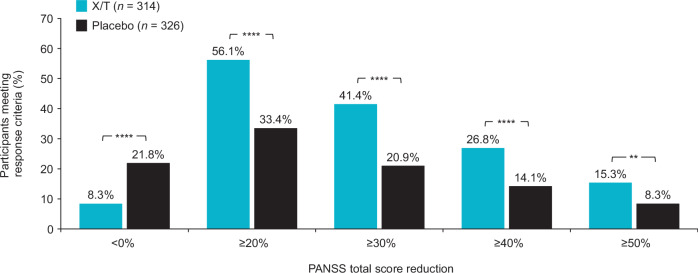
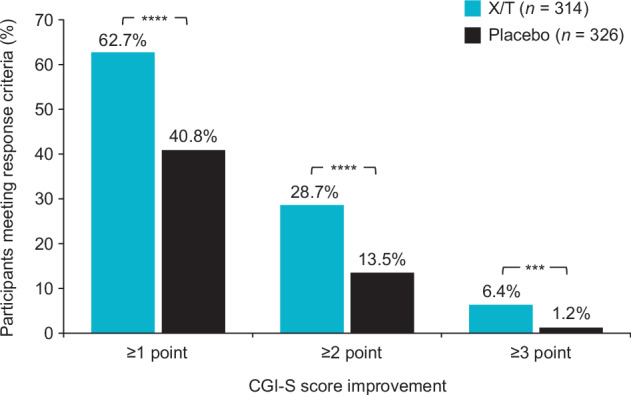
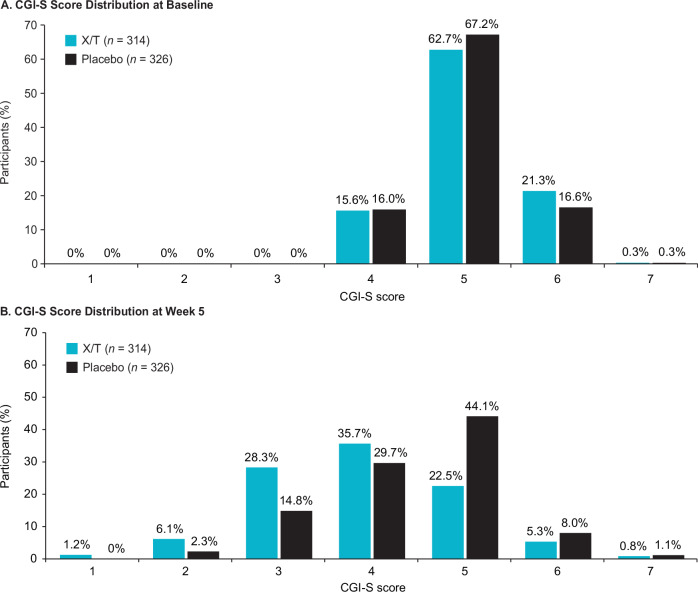
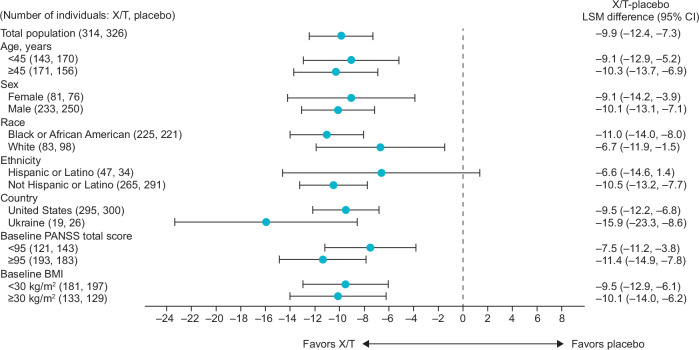
In the 5-week, randomized, double-blind, placebo-controlled EMERGENT-1 (NCT03697252), EMERGENT-2 (NCT04659161), and EMERGENT-3 (NCT04738123) trials, xanomeline and trospium chloride (formerly known as KarXT) significantly improved symptoms of schizophrenia and was generally well tolerated. We pooled data from the EMERGENT trials to further characterize the efficacy of xanomeline/trospium and provide sufficient statistical power to analyze responses in participant subgroups. In pooled analyses, xanomeline/trospium significantly improved Positive and Negative Syndrome Scale (PANSS) total score at week 5 versus placebo (least squares mean difference, -9.9; 95% confidence interval, -12.4, -7.3; p < 0.0001; Cohen's d effect size, 0.65). PANSS subscale and Clinical Global Impression-Severity scores also improved significantly with xanomeline/trospium versus placebo. Subgroup analyses consistently favored xanomeline/trospium over placebo regardless of differences in participant age, sex, race, body mass index, and baseline PANSS total score. These results add to existing evidence demonstrating robust and reliable improvements in symptoms with xanomeline/trospium across a broad spectrum of people with schizophrenia.
© 2024. The Author(s).
Conflict of interest statement
I.K., S.S., A.C., C.S., and H.Z. are employees of Karuna Therapeutics, a Bristol Myers Squibb company. A.C.M and S.K.B. are consultants of Karuna Therapeutics, a Bristol Myers Squibb company. H.H.H. was a principal investigator for the EMERGENT-1 and EMERGENT-2 trials. R.K. was a principal investigator for the EMERGENT-2 trial. L.C. is a consultant for AbbVie/Allergan, Acadia, Adamas, Alkermes, Angelini, Astellas, Avanir, Axsome, Biogen, BioXcel, Boehringer Ingelheim, Cadent Therapeutics, Cerevel, Clinilabs, COMPASS, Delpor, Eisai, Enteris BioPharma, HLS Therapeutics, Idorsia, INmune Bio, Impel, Intra-Cellular Therapies, Janssen, Karuna, Lundbeck, Luye, Lyndra, MapLight, Marvin, Medavante-ProPhase, Merck, Mitsubishi-Tanabe Pharma, Neumora, Neurocrine, Neurelis, Noema, Novartis, Noven, Otsuka, Ovid, Praxis, Recordati, Relmada, Reviva, Sage, Sumitomo/Sunovion, Supernus, Teva, University of Arizona, Vanda, Wells Fargo, and one-off ad hoc consulting for individuals/entities conducting marketing, commercial, or scientific scoping research; is a speaker for AbbVie/Allergan, Acadia, Alkermes, Angelini, Axsome, BioXcel, Eisai, Idorsia, Intra-Cellular Therapies, Janssen, Lundbeck, Neurocrine, Noven, Otsuka, Recordati, Sage, Sunovion, Takeda, Teva, and CME activities organized by medical education companies such as Medscape, NACCME, NEI, Vindico, and universities and professional organizations/societies; owns stocks (small number of shares of common stock) in Bristol-Myers Squibb, Eli Lilly, J & J, Merck, and Pfizer purchased >10 years ago, and stock options: Reviva; receives royalties/publishing income from Taylor & Francis (Editor-in-Chief,
Figures
References
-
- Indevus Pharmaceuticals. Sanctura (trospium chloride). Prescribing Information. 2012. Accessed 29 January 2024.
LinkOut - more resources
Full Text Sources
