

Biomarkers of glucose-insulin homeostasis and incident type 2 diabetes and cardiovascular disease: results from the Vitamin D and Omega-3 trial
- PMID: 39488682
- PMCID: PMC11531120
- DOI: 10.1186/s12933-024-02470-1
Biomarkers of glucose-insulin homeostasis and incident type 2 diabetes and cardiovascular disease: results from the Vitamin D and Omega-3 trial
Abstract
Background: Dysglycemia and insulin resistance increase type 2 diabetes (T2D) and cardiovascular disease (CVD) risk, yet associations with specific glucose-insulin homeostatic biomarkers have been inconsistent. Vitamin D and marine omega-3 fatty acids (n-3 FA) may improve insulin resistance. We sought to examine the association between baseline levels of insulin, C-peptide, HbA1c, and a novel insulin resistance score (IRS) with incident cardiometabolic diseases, and whether randomized vitamin D or n-3 FA modify these associations.
Methods: VITamin D and OmegA-3 TriaL (NCT01169259) was a randomized clinical trial testing vitamin D and n-3 FA for the prevention of CVD and cancer over a median of 5.3 years. Incident cases of T2D and CVD (including cardiovascular death, myocardial infarction, stroke, and coronary revascularization) were matched 1:1 on age, sex, and fasting status to controls. Conditional logistic regressions adjusted for demographic, clinical, and adiposity-related factors were used to assess the adjusted odds ratio (aOR) per-standard deviation (SD) and 95%CI of baseline insulin, C-peptide, HbA1c, and IRS (Insulin×0.0295 + C-peptide×0.00372) with risk of T2D, CVD, and coronary heart disease (CHD).
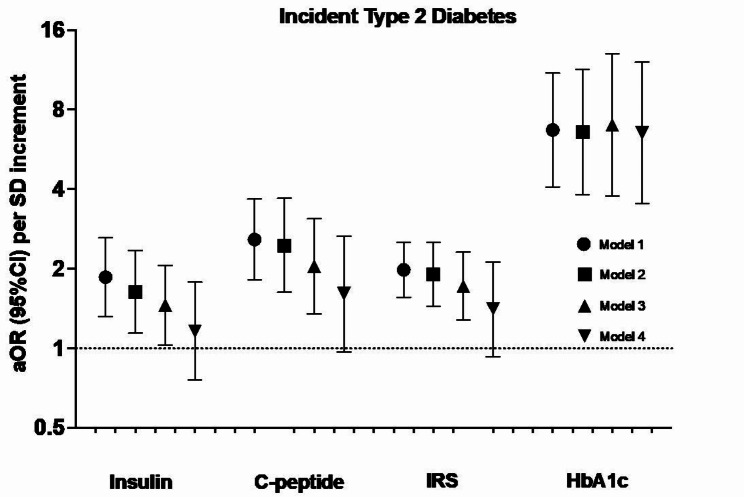
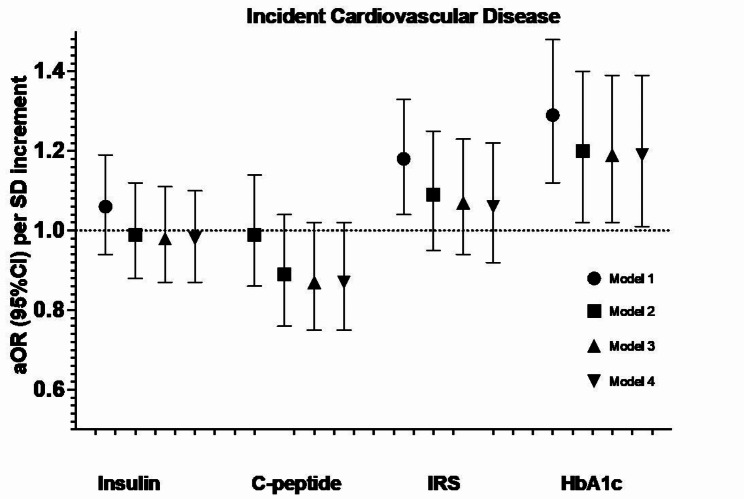
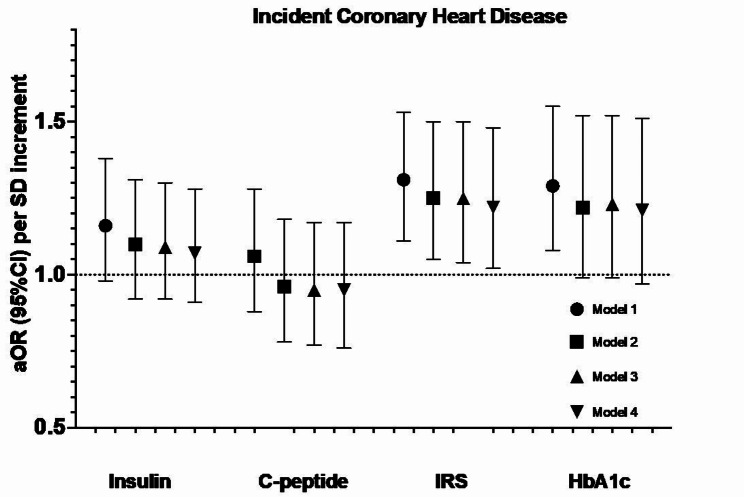
Results: We identified 218 T2D case-control pairs and 715 CVD case-control pairs including 423 with incident CHD. Each of the four biomarkers at baseline was separately associated with incident T2D, aOR (95%CI) per SD increment: insulin 1.46 (1.03, 2.06), C-peptide 2.04 (1.35, 3.09), IRS 1.72 (1.28, 2.31) and HbA1c 7.00 (3.76, 13.02), though only HbA1c remained statistically significant with mutual adjustments. For cardiovascular diseases, we only observed significant associations of HbA1c with CVD (1.19 [1.02, 1.39]), and IRS with CHD (1.25 [1.04, 1.50]), which persisted after mutual adjustment. Randomization to vitamin D and/or n-3 FA did not modify the association of these biomarkers with the endpoints.
Conclusions: Each of insulin, C-peptide, IRS, and HbA1c were associated with incident T2D with the strongest association noted for HbA1c. While HbA1c was significantly associated with CVD risk, a novel IRS appears to be associated with CHD risk. Neither vitamin D nor n-3 FA modified the associations between these biomarkers and cardiometabolic outcomes.
Keywords: Cardiovascular disease; Insulin resistance; Omega-3 fatty acids; Type 2 diabetes; Vitamin D.
© 2024. The Author(s).
Conflict of interest statement
JL, JB, and MJM are Quest Diagnostics employees and/or have stock ownership. SM served as a consultant to Pfizer outside the current work. The other authors declare no relevant conflicts of interest.
Figures
References
-
- Kurl S, Zaccardi F, Onaemo VN, Jae SY, Kauhanen J, Ronkainen K, et al. Association between HOMA-IR, fasting insulin and fasting glucose with coronary heart disease mortality in nondiabetic men: a 20-year observational study. Acta Diabetol. 2015;52(1):183–6. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
