

Dyslipidemia in Juvenile Dermatomyositis
- PMID: 39489760
- PMCID: PMC11532421
- DOI: 10.1038/s41598-024-77985-4
Dyslipidemia in Juvenile Dermatomyositis
Abstract
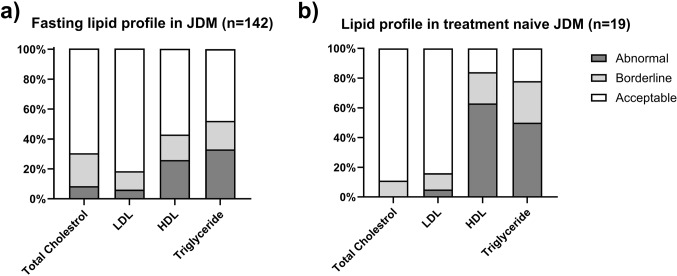
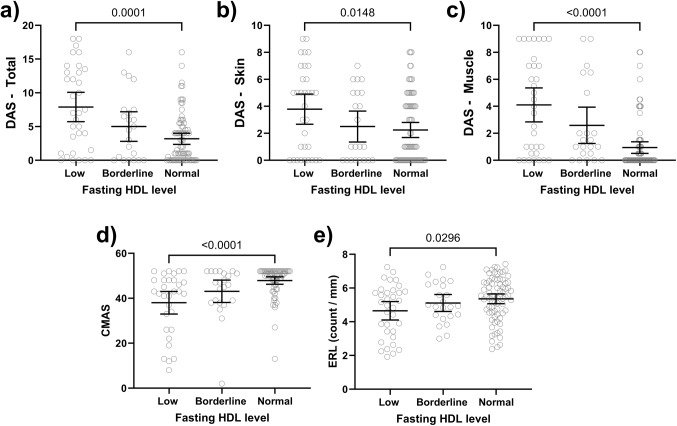
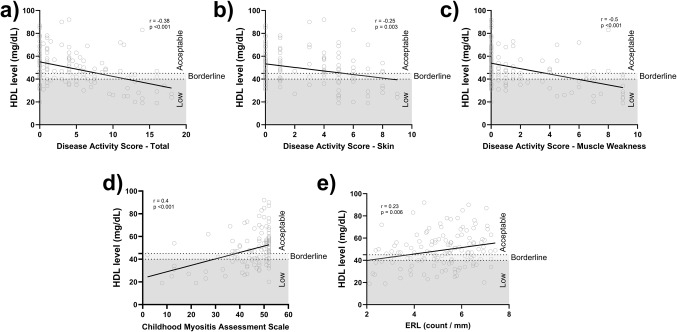
This study investigates the prevalence of dyslipidemia and its association with disease activity in children with Juvenile Dermatomyositis (JDM). A retrospective chart review of 142 JDM patients who had fasting lipid profiles was conducted. Clinical, and laboratory indicators of disease activity at the time of lipid assessment were obtained. JDM patients displayed a high prevalence (72%) of abnormal or borderline fasting lipid profiles, particularly involving HDL and triglycerides. Treatment-naïve patients exhibited the most significant dyslipidemia, with significantly lower median HDL levels compared to those on medication (30 vs. 49 mg/dL, p < 0.0001). HDL levels inversely correlated with various disease activity measures, including disease activity score (DAS) total (r= -0.38, p < 0.001), DAS muscle weakness (r= -0.5, p < 0.001), DAS skin (r= -0.25, p = 0.003), neopterin (r= -0.41, p < 0.001), ESR (r= -0.25, p = 0.006), and vWF Ag (r= -0.21, p = 0.02). In conclusion, JDM patients have a high prevalence of dyslipidemia, especially low HDL and elevated triglycerides. The severity of dyslipidemia (low HDL) correlates with disease activity, with treatment-naïve patients demonstrating the lowest HDL levels. These findings suggest the importance of annual lipid profile monitoring in JDM patients, potentially followed by early interventions such as dietary adjustments and exercise programs.
Keywords: Disease Activity scores; Dyslipidemia; HDL; Juvenile Dermatomyositis; Neopterin.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

References
-
- Mendez, E. P. et al. US incidence of juvenile dermatomyositis, 1995–1998: results from the National Institute of Arthritis and Musculoskeletal and skin diseases Registry. Arthritis Rheum.49, 300–305. 10.1002/art.11122 (2003). - PubMed
-
- Marie, I. Morbidity and mortality in adult polymyositis and dermatomyositis. Curr. Rheumatol. Rep.14, 275–285. 10.1007/s11926-012-0249-3 (2012). - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
