

Comparative effectiveness and safety of escalating to triple therapy versus switching to dual bronchodilators after discontinuing LABA/ICS in patients with COPD: a retrospective cohort study
- PMID: 39491813
- PMCID: PMC11533288
- DOI: 10.1177/17534666241292242
Comparative effectiveness and safety of escalating to triple therapy versus switching to dual bronchodilators after discontinuing LABA/ICS in patients with COPD: a retrospective cohort study
Abstract
Background: The latest guidelines discourage the use of long-acting beta2-agonists/inhaled corticosteroids (LABA/ICS) for chronic obstructive pulmonary disease (COPD). However, there is a lack of evidence regarding the optimal subsequent treatment after discontinuing LABA/ICS.
Objectives: To compare the effectiveness and safety of switching from LABA/ICS to triple therapy (LABA/long-acting muscarinic antagonists (LAMA)/ICS) or to dual bronchodilators (LABA/LAMA) in COPD patients.
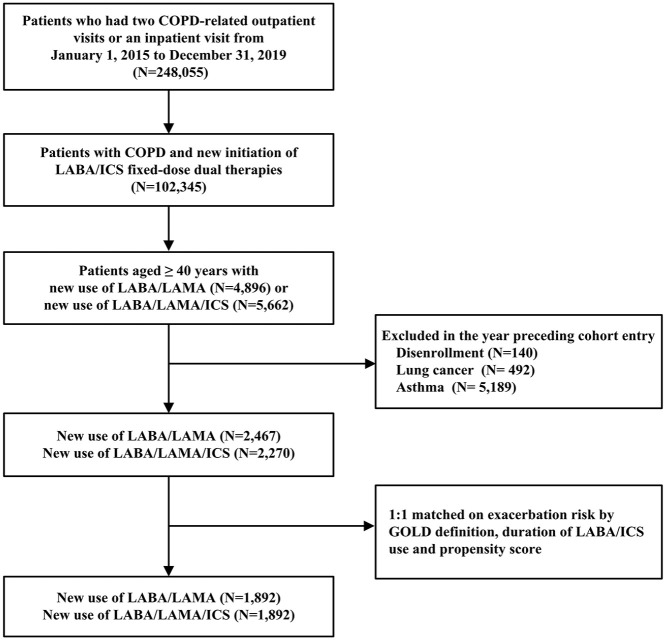
Design: This was a new-user, active-comparator, and propensity score-matched cohort study analyzing the Taiwanese nationwide healthcare insurance claims.
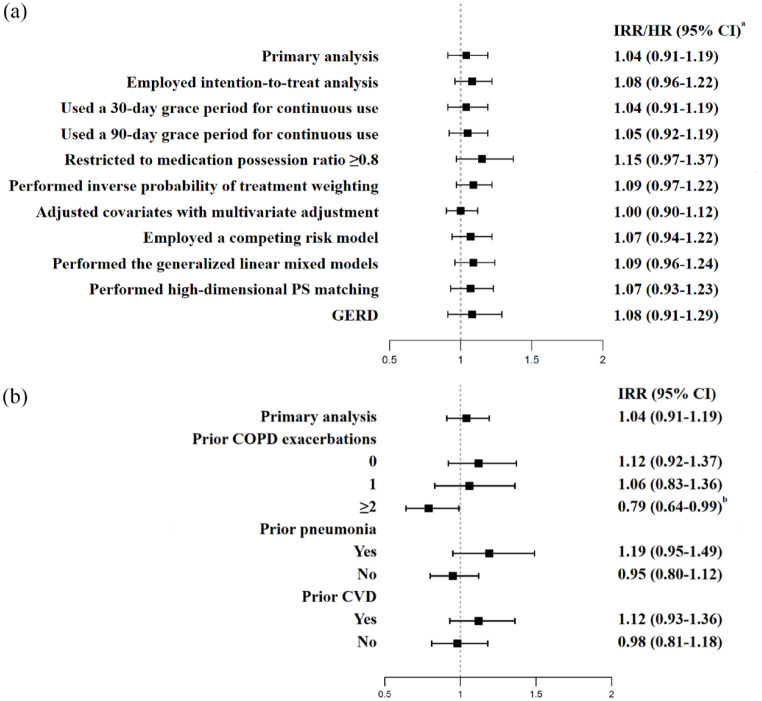
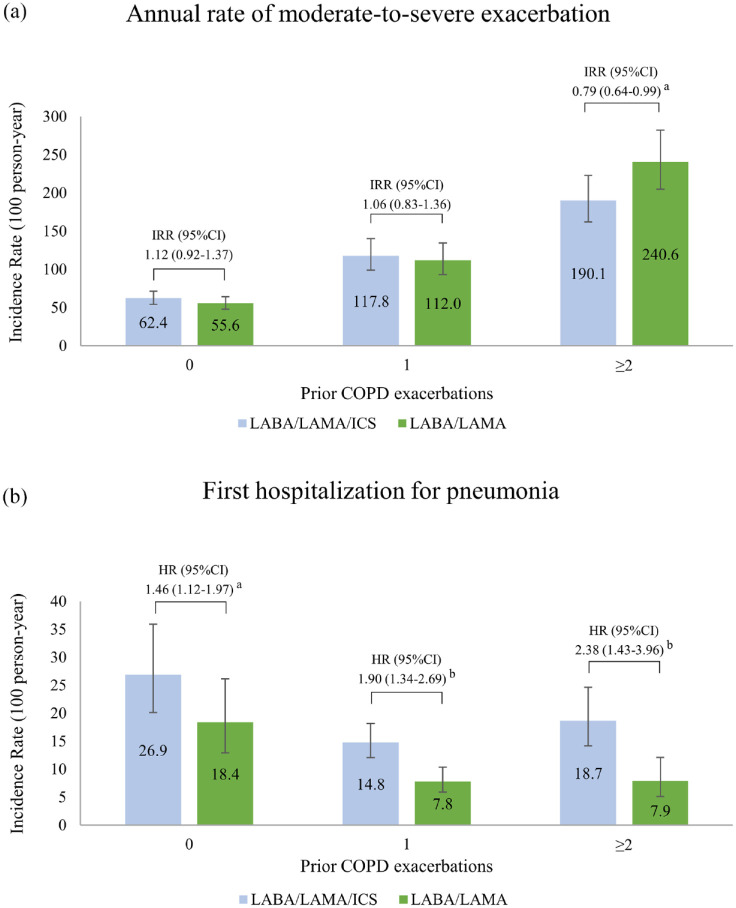
Methods: We recruited COPD patients switching from LABA/ICS to triple therapy or to dual bronchodilators from 2015 to 2019. The primary effectiveness outcome was the annual rate of exacerbations, and safety outcomes included severe pneumonia and all-cause mortality. Stratification by prior exacerbations was conducted.
Results: After matching, each group comprised 1892 patients, 55% of whom experienced no exacerbations in the prior year. Treatment with LABA/LAMA/ICS versus LABA/LAMA showed comparable annual rate of moderate-to-severe exacerbations (incidence rate ratio, 1.04; 95% confidence interval (CI), 0.91-1.19). However, switching to LABA/LAMA/ICS was associated with increased risks of severe pneumonia (hazard ratio (HR), 1.65; 95% CI, 1.30-2.09) and all-cause death (HR, 1.39; 95% CI, 1.09-1.78). In patients with⩾2 prior exacerbations, LABA/LAMA/ICS versus LABA/LAMA was related to a 21% reduced rate of exacerbations but with a twofold increased pneumonia risk and a 49% elevated risk of all-cause mortality.
Conclusion: Switching from LABA/ICS to triple therapy versus dual bronchodilators in COPD patients was associated with similar rates of annual exacerbations but was related to elevated risks of severe pneumonia and all-cause mortality. Among frequent exacerbators, triple therapy was associated with lower rates of exacerbation but was accompanied by increased risks of pneumonia and mortality compared to LABA/LAMA. Careful consideration of the examined safety events is necessary when switching from LABA/ICS to triple therapy in COPD management.
Keywords: COPD; comparative effectiveness and safety; dual therapy; observational study; triple therapy.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Figures
References
-
- Aaron SD, Donaldson G, Whitmore GA, et al. Time course and pattern of COPD exacerbation onset. Thorax 2012; 67(3): 238–243. - PubMed
-
- Global Initiative for Chronic Obstructive Lung Disease. Global strategy for the diagnosis, management and prevention of chronic obstructive pulmonary disease: 2024 report. Global initiative for chronic obstructive lung disease website, https://goldcopd.org/2024-gold-report/ (2024, accessed 15 May 2024).
-
- Lareau S, Moseson E, Slatore CG. Exacerbation of COPD. Am J Respir Crit Care Med 2018; 198(11): 21–22. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
