

Hormones in malaria infection: influence on disease severity, host physiology, and therapeutic opportunities
- PMID: 39492784
- PMCID: PMC11581842
- DOI: 10.1042/BSR20240482
Hormones in malaria infection: influence on disease severity, host physiology, and therapeutic opportunities
Abstract
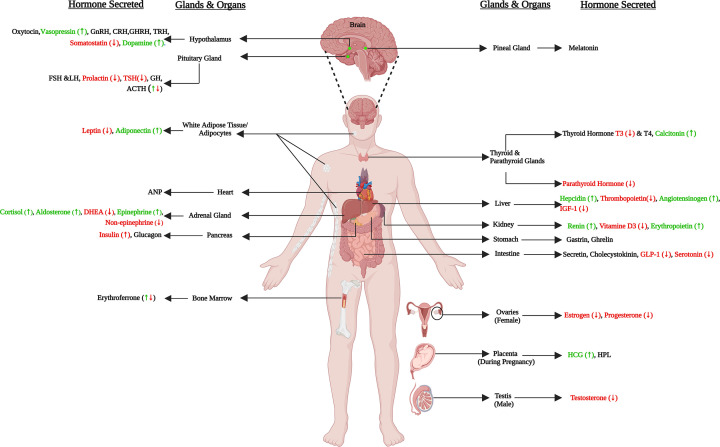
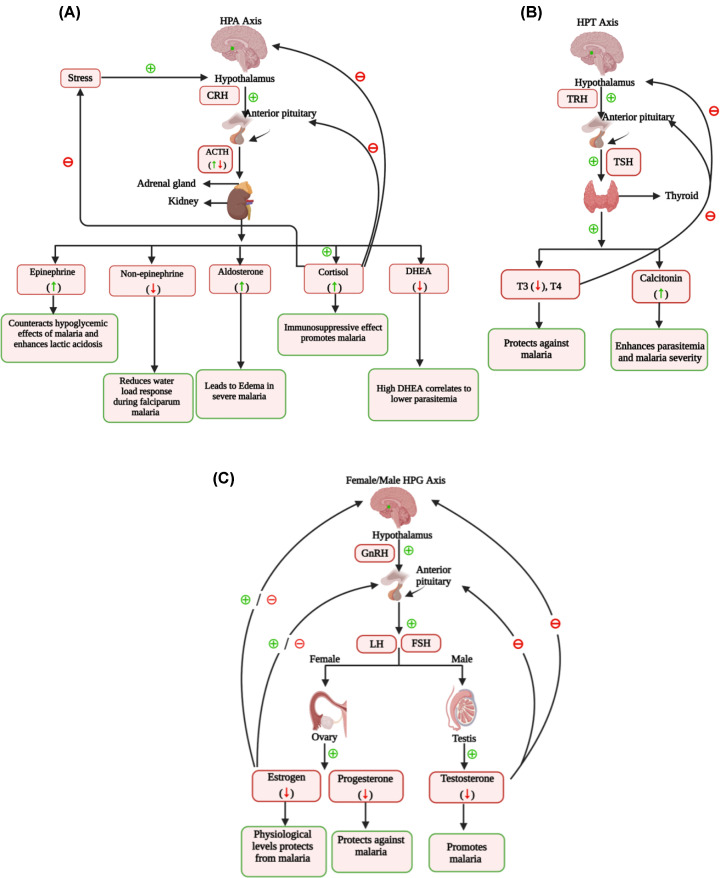
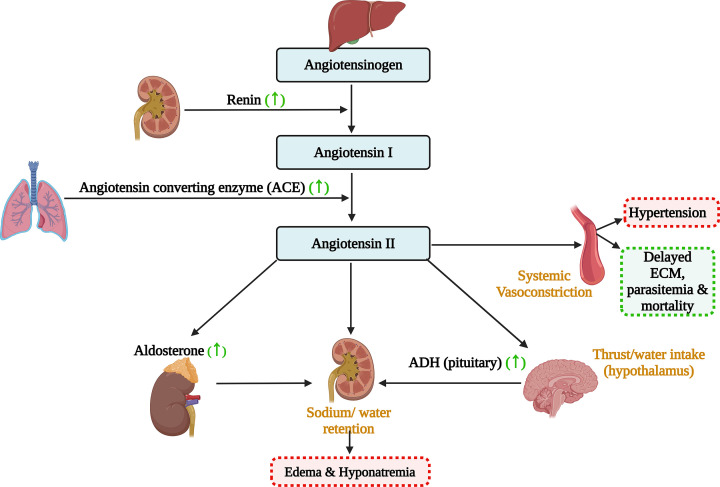
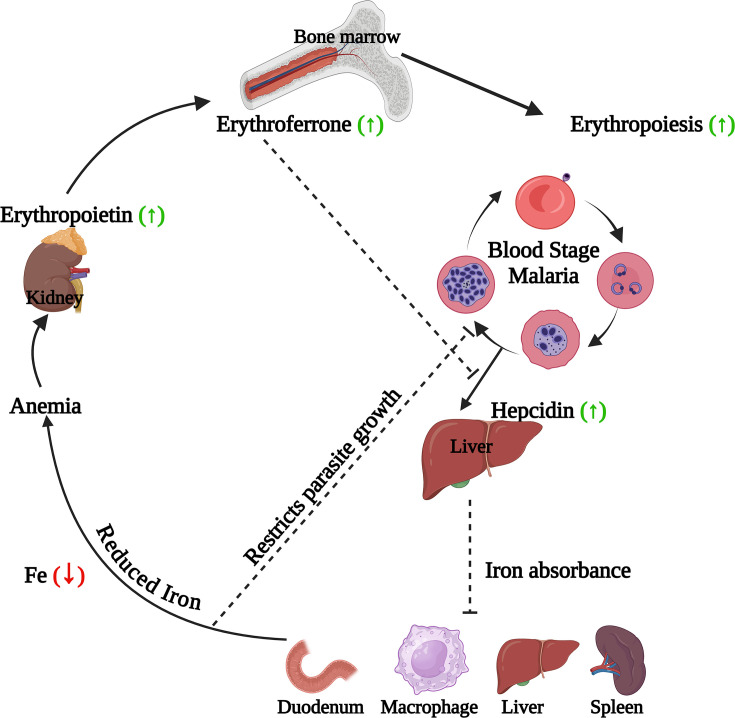
Human malaria, caused by Plasmodium parasites, is a fatal disease that disrupts the host's physiological balance and affects the neuroendocrine system. This review explores how malaria influences and is influenced by hormones. Malaria activates the Hypothalamus-Pituitary-Adrenal axis, leading to increased cortisol, aldosterone, and epinephrine. Cortisol, while reducing inflammation, aids parasite survival, whereas epinephrine helps manage hypoglycemia. The Hypothalamus-Pituitary-Gonad and Hypothalamus-Pituitary-Thyroid axes are also impacted, resulting in lower sex and thyroid hormone levels. Malaria disrupts the renin-angiotensin-aldosterone system (RAAS), causing higher angiotensin-II and aldosterone levels, contributing to edema, hyponatremia and hypertension. Malaria-induced anemia is exacerbated by increased hepcidin, which impairs iron absorption, reducing both iron availability for the parasite and red blood cell formation, despite elevated erythropoietin. Hypoglycemia is common due to decreased glucose production and hyperinsulinemia, although some cases show hyperglycemia due to stress hormones and inflammation. Hypocalcemia, and hypophosphatemia are associated with low Vitamin D3 and parathyroid hormone but high calcitonin. Hormones such as DHEA, melatonin, PTH, Vitamin D3, hepcidin, progesterone, and erythropoietin protects against malaria. Furthermore, synthetic analogs, receptor agonists and antagonists or mimics of hormones like DHEA, melatonin, serotonin, PTH, vitamin D3, estrogen, progesterone, angiotensin, and somatostatin are being explored as potential antimalarial treatments or adjunct therapies. Additionally, hormones like leptin and PCT are being studied as probable markers of malaria infection.
Keywords: Human hormones; Plasmodium; antimalarial; host-pathogen interactions; malaria.
© 2024 The Author(s).
Conflict of interest statement
The authors declare that there are no competing interests associated with the manuscript.
Figures
Similar articles
-
Primaquine for reducing Plasmodium falciparum transmission.Cochrane Database Syst Rev. 2012 Sep 12;(9):CD008152. doi: 10.1002/14651858.CD008152.pub2. Cochrane Database Syst Rev. 2012. Update in: Cochrane Database Syst Rev. 2014 Jun 30;(6):CD008152. doi: 10.1002/14651858.CD008152.pub3. PMID: 22972117 Updated.
-
Proteomes of plasmodium knowlesi early and late ring-stage parasites and infected host erythrocytes.J Proteomics. 2024 Jun 30;302:105197. doi: 10.1016/j.jprot.2024.105197. Epub 2024 May 15. J Proteomics. 2024. PMID: 38759952 Free PMC article.
-
The Black Book of Psychotropic Dosing and Monitoring.Psychopharmacol Bull. 2024 Jul 8;54(3):8-59. Psychopharmacol Bull. 2024. PMID: 38993656 Free PMC article. Review.
-
EORTC guidelines for the use of erythropoietic proteins in anaemic patients with cancer: 2006 update.Eur J Cancer. 2007 Jan;43(2):258-70. doi: 10.1016/j.ejca.2006.10.014. Epub 2006 Dec 19. Eur J Cancer. 2007. PMID: 17182241
-
Systemic Inflammatory Response Syndrome.2025 Jun 20. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. 2025 Jun 20. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMID: 31613449 Free Books & Documents.
Cited by
-
Micronutrient Biomarkers and Their Association with Malaria Infection in Children in Buea Health District, Cameroon.Trop Med Infect Dis. 2024 Dec 10;9(12):303. doi: 10.3390/tropicalmed9120303. Trop Med Infect Dis. 2024. PMID: 39728830 Free PMC article.
-
The Immunomodulatory Role of Estrogen in Malaria: A Review of Sex Differences and Therapeutic Implications.Immun Inflamm Dis. 2025 Feb;13(2):e70148. doi: 10.1002/iid3.70148. Immun Inflamm Dis. 2025. PMID: 39898752 Free PMC article. Review.
References
-
- (2023) World malaria report. https://www.who.int/teams/global-malaria-programme/reports/world-malaria...
-
- Ogbera A.O. and Anaba E. (2021) Protozoa and Endocrine Dysfunction. Endotext, MDText.com, Inc
-
- Stelzer I.A. and Arck P.C. (2016) Immunity and the Endocrine System. 10.1016/B978-0-12-374279-7.19001-0 - DOI
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical