

Prognostic role of lipoprotein(a) in atherosclerotic cardiovascular disease risk from a perspective on current risk stratification
- PMID: 39492837
- PMCID: PMC11527816
- DOI: 10.1002/mco2.773
Prognostic role of lipoprotein(a) in atherosclerotic cardiovascular disease risk from a perspective on current risk stratification
Abstract
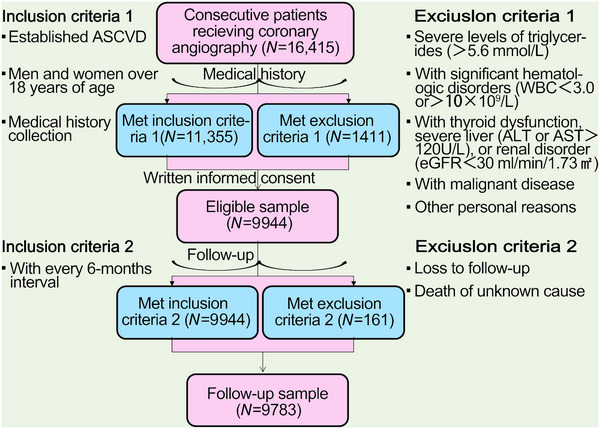
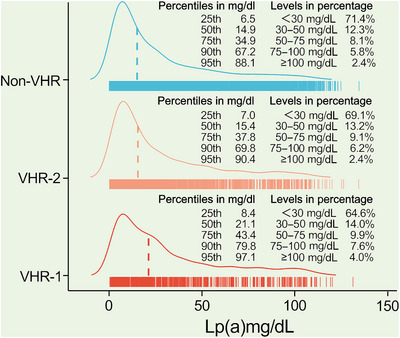
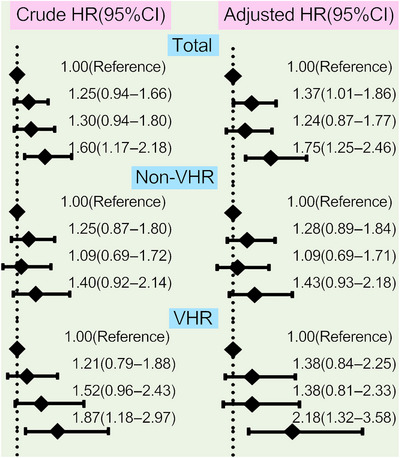
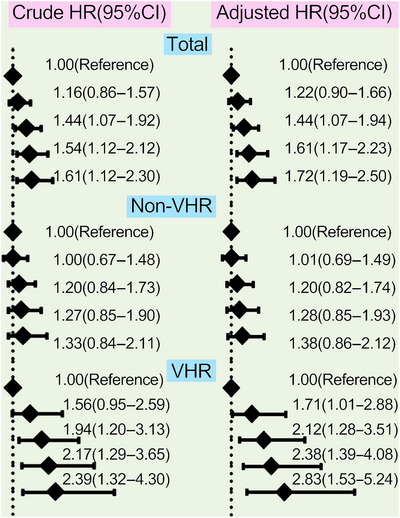
Lipoprotein(a) [Lp(a)] is an emerging predictor for atherosclerotic cardiovascular disease (ASCVD) but the association from a perspective on current risk stratification was unknown. A cohort of 9944 Chinese patients with ASCVD was recruited and refined into very-high-risk (VHR) and non-VHR subgroups according to current guideline. Lp(a) plasma levels were divided by its concentration (<30, 30-50, 50-75, and ≥75 mg/dL) and percentile zones (<25th, 25-50th, 50-75th, 75-90th, ≥90th). Cardiovascular events (CVEs) occurred during an average of 38.5 months' follow-up were recorded. We found that Lp(a) was increased with risk stratification of ASCVD increasing. Prevalence of CVEs had a significantly increasing trend with gradients of Lp(a) elevation in VHR but not in non-VHR subgroup. The adjusted HRs (95%CIs) for CVEs were 1.75(1.25-2.46) in the highest group of Lp(a) ≥75 mg/dL compared with the group of Lp(a) <30 mg/dL as the reference in overall patients, 2.18(1.32-3.58) in VHR subgroup and 1.43(0.93-2.18) in non-VHR subgroup, respectively. The adjusted HRs (95%CIs) at the highest grade of Lp(a) levels (≥90th) were 1.72(1.19-2.50) in overall population, 2.83(1.53-5.24) in VHR subgroup and 1.38(0.86-2.12) in non-VHR subgroup, respectively. These findings suggested that Lp(a) might contribute more to CVEs risk in VHR subgroup of ASCVD.
Keywords: Chinese; atherosclerotic cardiovascular disease; lipoprotein(a); risk stratification.
© 2024 The Author(s). MedComm published by Sichuan International Medical Exchange & Promotion Association (SCIMEA) and John Wiley & Sons Australia, Ltd.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Figures

References
-
- Gencer B, Kronenberg F, Stroes ES, Mach F. Lipoprotein(a): the revenant. Eur Heart J. 2017;38(20):1553‐1560. - PubMed
-
- Sandholzer C, Saha N, Kark JD, et al. Apo(a) isoforms predict risk for coronary heart disease. A study in six populations. Arterioscler Thromb. 1992;12(10):1214‐1226. - PubMed
-
- Kamstrup PR, Tybjaerg‐Hansen A, Steffensen R, Nordestgaard BG. Genetically elevated lipoprotein(a) and increased risk of myocardial infarction. JAMA. 2009;301(22):2331‐2339. - PubMed
-
- Tsimikas S. A Test in Context: lipoprotein(a): diagnosis, prognosis, controversies, and emerging therapies. J Am Coll Cardiol. 2017;69(6):692‐711. - PubMed
-
- Ruscica M, Sirtori CR, Corsini A, et al. Lipoprotein(a): knowns, unknowns and uncertainties. Pharmacol Res. 2021;173:105812. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous