

Apixaban and Limiting Aspirin for Patients With Atrial Fibrillation, Percutaneous Coronary Intervention, and Multimorbidity
- PMID: 39493312
- PMCID: PMC11530834
- DOI: 10.1016/j.jacadv.2024.101335
Apixaban and Limiting Aspirin for Patients With Atrial Fibrillation, Percutaneous Coronary Intervention, and Multimorbidity
Abstract
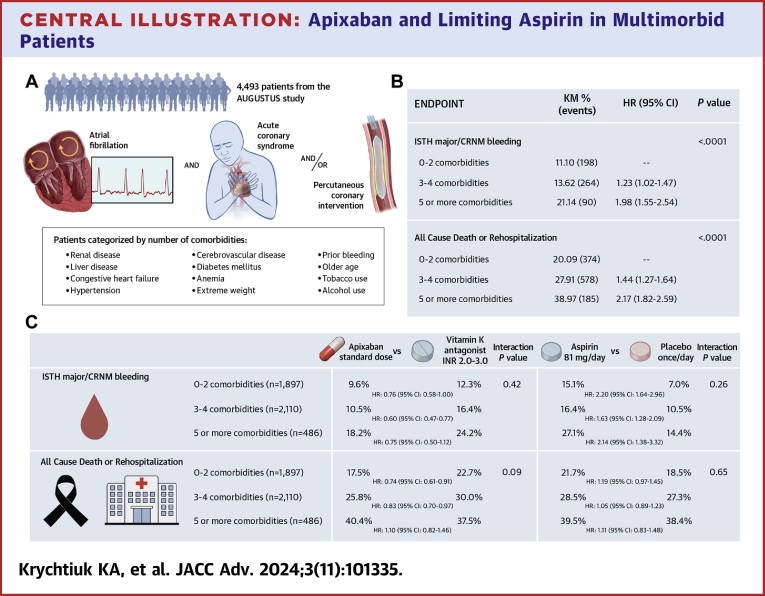
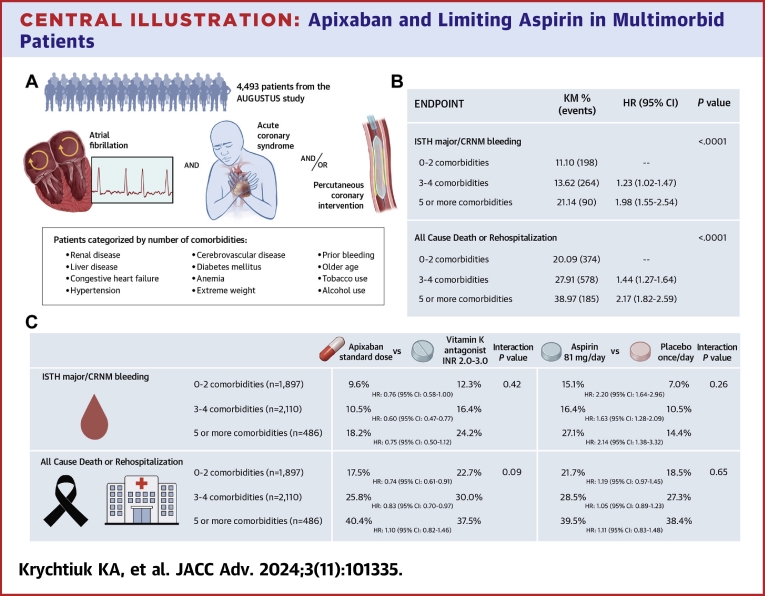
Background: Patients with atrial fibrillation (AF) after an acute coronary syndrome (ACS) and/or undergoing percutaneous coronary intervention (PCI) with multiple comorbidities are at increased risk for bleeding and ischemic events.
Objectives: This post-hoc analysis of AUGUSTUS describes the safety and efficacy of antithrombotic regimens in patients with multimorbidity.
Methods: AUGUSTUS was a 2 × 2 factorial, randomized controlled trial evaluating the safety of apixaban vs vitamin K antagonists (VKA) (open-label) and aspirin vs placebo (double-blind) in patients with AF and ACS and/or PCI treated with a P2Y12 inhibitor. Patients were categorized as having no multimorbidity (0-2 comorbidities), moderate multimorbidity (3-4 comorbidities), or high multimorbidity (≥5 comorbidities). The associations between multimorbidity and clinical outcomes and interactions with antithrombotic regimens were tested.
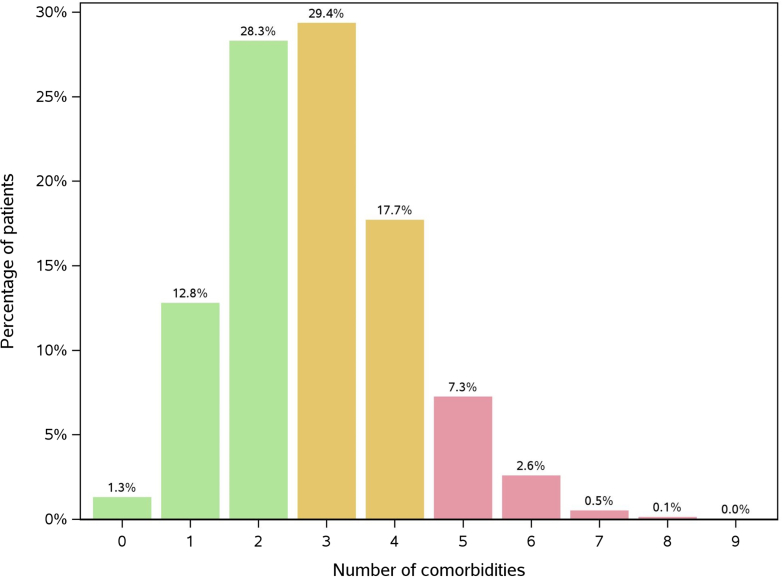
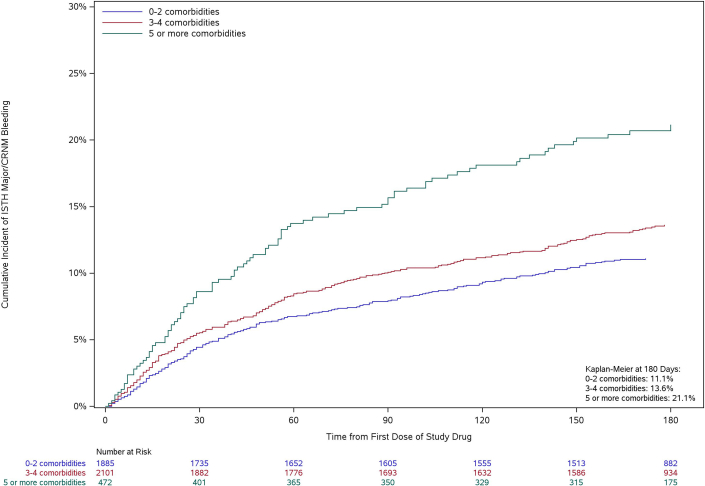
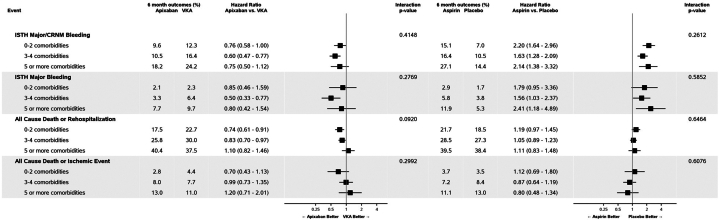
Results: Of 4,493 patients (97.4%) with available comorbidity data, 1,897 (42.2%) had no multimorbidity, 2,110 (47%) had moderate, and 486 (10.8%) had high multimorbidity. Patients with moderate (HR: 1.23; 95% CI: 1.02-1.47) and high (HR: 1.98; 95% CI: 1.55-2.54) multimorbidity had higher rates of International Society on Thrombosis and Haemostasis (ISTH) major or clinically relevant nonmajor (CRNM) bleeding compared to patients with no multimorbidity. No significant interaction between multimorbidity and apixaban vs vitamin K antagonists was observed for ISTH major bleeding/CRNM (P int = 0.415), death or hospitalization (P int = 0.092), or death or ischemic event (P int = 0.299). Similarly, no significant interaction between multimorbidity and aspirin vs placebo was seen for ISTH major bleeding/CRNM (P int = 0.261), death or hospitalization (P int = 0.646), or death or ischemic event (P int = 0.608).
Conclusions: Our findings support the standard use of apixaban plus a P2Y12 inhibitor in patients with AF and ACS/PCI, irrespective of the presence of multimorbidity.
Keywords: PCI; anticoagulation; apixaban; aspirin; atrial fibrillation; bleeding; multimorbidity.
© 2024 The Authors.
Conflict of interest statement
The AUGUSTUS trial and this analysis were supported by Bristol Myers Squibb and 10.13039/100004319Pfizer. Dr Krychtiuk was supported by a research grant from the 10.13039/100015330Max Kade Foundation/10.13039/501100001822Austrian Academy of Science. Dr Krychtiuk has received speaker fees from Daiichi Sankyo and Zoll Medical; consulting fees from Amarin, Novartis, and Sanofi; and travel support from 10.13039/100002429Amgen and 10.13039/100004339Sanofi. Dr Lopes has received research grants or contracts from Amgen, Bristol-Myers Squibb, GlaxoSmithKline, Medtronic, Pfizer, and Sanofi-Aventis; funding for educational activities or lectures from Pfizer, Daiichi Sankyo, and Novo Nordisk; and funding for consulting or other services from Bayer, Boehringer Ingelheim, Bristol-Myers Squibb, and Novo Nordisk. Dr Goodman has received research grant support (eg, steering committee or data and safety monitoring committee) and/or speaker/consulting honoraria (eg, advisory boards) from Amgen, Anthos Therapeutics, AstraZeneca, Bayer, Boehringer Ingelheim, Bristol Myers Squibb, CSL Behring, CYTE Ltd, Daiichi-Sankyo/American Regent, Eli Lilly, Esperion, Ferring Pharmaceuticals, HLS Therapeutics, Idorsia, JAMP Pharma, Merck, Novartis, Novo Nordisk A/C, Pendopharm/Pharmascience, Pfizer, Regeneron, Sanofi, Servier, Tolmar Pharmaceuticals, Valeo Pharma; and salary support/honoraria from the Heart and Stroke Foundation of Ontario/University of Toronto (Polo) Chair, Canadian Heart Failure Society, Canadian Heart Research Centre and MD Primer, Canadian VIGOUR Centre, Cleveland Clinic Coordinating Centre for Clinical Research, Duke Clinical Research Institute, New York University Clinical Coordinating Centre, PERFUSE Research Institute, and TIMI Study Group (Brigham Health). Dr Aronson is an employee of Bristol Myers Squibb. Dr Windecker has received research, travel, or educational grants to the institution without personal remuneration from Abbott, Abiomed, Amgen, Astra Zeneca, Bayer, Braun, Biotronik, Boehringer Ingelheim, Boston Scientific, Bristol Myers Squibb, Cardinal Health, CardioValve, Cordis Medical, Corflow Therapeutics, CSL Behring, Daiichi Sankyo, Edwards Lifesciences, Farapulse Inc, Fumedica, Guerbet, Idorsia, Inari Medical, InfraRedx, Janssen-Cilag, Johnson & Johnson, Medalliance, Medicure, Medtronic, Merck Sharp & Dohm, Miracor Medical, MonarQ, Novartis, Novo Nordisk, Organon, OrPha Suisse, Pharming Tech, Pfizer, Polares, Regeneron, Sanofi-Aventis, Servier, Sinomed, Terumo, Vifor, and V-Wave. Dr Windecker served as an advisory board member and/or member of the steering/executive group of trials funded by 10.13039/100000046Abbott, 10.13039/100020297Abiomed, 10.13039/100002429Amgen, Astra Zeneca, 10.13039/100004326Bayer, 10.13039/100008497Boston Scientific, 10.13039/501100005035Biotronik, Bristol Myers Squibb, 10.13039/100006520Edwards Lifesciences, 10.13039/501100023518MedAlliance, 10.13039/100004374Medtronic, 10.13039/100004336Novartis, Polares, Recardio, Sinomed, 10.13039/501100008645Terumo, and V-Wave with payments to the institution but no personal payments; and he is a member of the steering/executive committee group of several investigator-initiated trials that receive funding from industry without impacting his personal remuneration. Dr Mehran has received institutional research payments from: Abbott, Abiomed, Affluent Medical, Alleviant Medical, Amgen, AM-Pharma, Arena, AstraZeneca, AtriCure Inc, Biosensors, Biotronik, Boston Scientific, Bristol-Myers Squibb, CardiaWave, CeloNova, CERC, Chiesi, Concept Medical, Cytosorbents, Daiichi Sankyo, Duke, Element Science, Essential Medical, Faraday, Idorsia Pharmaceuticals, Janssen, MedAlliance, Mediasphere, Medtelligence, Medtronic, MJH Healthcare, Novartis, OrbusNeich, Penumbra, PhaseBio, Philips, Pi-Cardia, PLx Pharma, Population Health Research Institute, Protembis, RecCor Medical Inc, RenalPro, RM Global, Sanofi, Shockwave, Vivasure, Zoll; personal fees from Cardiovascular Research Foundation (CRF), Cordis, Daiichi Sankyo Brasil, E.R. Squibb & Sons, Esperion Science/Innovative Biopharma, Europa Group/Boston Scientific, Gaffney Events, Educational Trust, Henry Ford Health Cardiology, Ionis Pharmaceuticals, MedCon International, Novartis, NovoNordisk, PeerView Institute for Medical Education, TERUMO Europe N.V., Vectura, VoxMedia, WebMD, IQVIA, Radcliffe, and TARSUS Cardiology; no fees from AMA (Scientific Advisory Board) and SCAI (Women in Innovations Committee Member); and Faculty CRF Honorarium: JAMA Cardiology (Associate Editor) and ACC (BOT Member, SC Member CTR Program). Dr Granger has received consulting fees from Abbvie, Abiomed, Alnylam, Anthos, Bayer, Boehringer Ingelheim, Boston Scientific, Bristol Myers Squibb, Cardionomic, Celecor Therapeutics, Hengrui USA, Janssen, Medscape, Medtronic, Merck, NephroSynergy, Novo Nordisk, NIH, Novartis, Pfizer, Philips, REATA, Roche, and Veralox Therapeutics Inc; grants/contracts from Alnylam, Boehringer Ingelheim, Bristol Myers Squibb, Duke Clinical Research Institute, FDA, Janssen, Lilly, Novartis, Pfizer, and Philips; equity from Tenac.io. Dr Alexander has received research grants through Duke University from Artivion/CryoLife, Bayer, Bristol-Myers Squibb, CSL Behring, Ferring, the U.S. FDA, Humacyte, and the U.S. NIH, and advisory board or consulting payments from AbbVie, Akros, Artivion/CryoLife, AtriCure, Bayer, Bristol-Myers Squibb, Ferring, GlaxoSmithKline, Janssen, Novostia, Pfizer, Portola, Theravance, and Veralox.
Figures
Similar articles
-
Antithrombotic Therapy to Minimize Total Events After ACS or PCI in Atrial Fibrillation: Insights From AUGUSTUS.J Am Coll Cardiol. 2025 Mar 25;85(11):1157-1168. doi: 10.1016/j.jacc.2024.10.125. Epub 2025 Feb 5. J Am Coll Cardiol. 2025. PMID: 39918467 Clinical Trial.
-
Antithrombotic Therapy in Patients With Atrial Fibrillation and Acute Coronary Syndrome Treated Medically or With Percutaneous Coronary Intervention or Undergoing Elective Percutaneous Coronary Intervention: Insights From the AUGUSTUS Trial.Circulation. 2019 Dec 3;140(23):1921-1932. doi: 10.1161/CIRCULATIONAHA.119.043308. Epub 2019 Sep 26. Circulation. 2019. PMID: 31557056 Clinical Trial.
-
Apixaban or Warfarin and Aspirin or Placebo After Acute Coronary Syndrome or Percutaneous Coronary Intervention in Patients With Atrial Fibrillation and Prior Stroke: A Post Hoc Analysis From the AUGUSTUS Trial.JAMA Cardiol. 2022 Jul 1;7(7):682-689. doi: 10.1001/jamacardio.2022.1166. JAMA Cardiol. 2022. PMID: 35612866 Free PMC article. Clinical Trial.
-
Safety and efficacy of double vs. triple antithrombotic therapy in patients with atrial fibrillation with or without acute coronary syndrome undergoing percutaneous coronary intervention: a collaborative meta-analysis of non-vitamin K antagonist oral anticoagulant-based randomized clinical trials.Eur Heart J Cardiovasc Pharmacother. 2021 Apr 9;7(FI1):f50-f60. doi: 10.1093/ehjcvp/pvaa116. Eur Heart J Cardiovasc Pharmacother. 2021. PMID: 33119069 Free PMC article.
-
The role of triple antithrombotic therapy in patients with atrial fibrillation undergoing percutaneous coronary intervention.Prog Cardiovasc Dis. 2021 Nov-Dec;69:11-17. doi: 10.1016/j.pcad.2021.11.010. Epub 2021 Dec 6. Prog Cardiovasc Dis. 2021. PMID: 34883097 Review.
References
-
- Tsao C.W., Aday A.W., Almarzooq Z.I., et al. Heart disease and stroke statistics-2023 update: a report from the American heart association. Circulation. 2023;147:e93–e621. - PubMed
-
- Fanaroff A.C., Li S., Marquis-Gravel G., et al. Atrial fibrillation and coronary artery disease: a long-term perspective on the need for combined antithrombotic therapy. Circ Cardiovasc Interv. 2021;14 - PubMed
-
- Hindricks G., Potpara T., Dagres N., et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): the Task Force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) Developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur Heart J. 2021;42:373–498. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
