

Integrating Big Data, Artificial Intelligence, and motion analysis for emerging precision medicine applications in Parkinson's Disease
- PMID: 39493349
- PMCID: PMC11525280
- DOI: 10.1186/s40537-024-01023-3
Integrating Big Data, Artificial Intelligence, and motion analysis for emerging precision medicine applications in Parkinson's Disease
Abstract
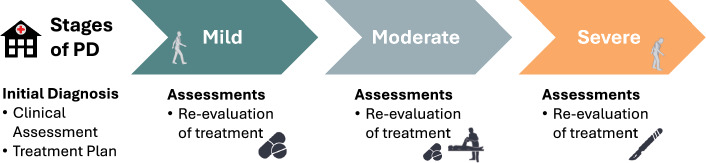
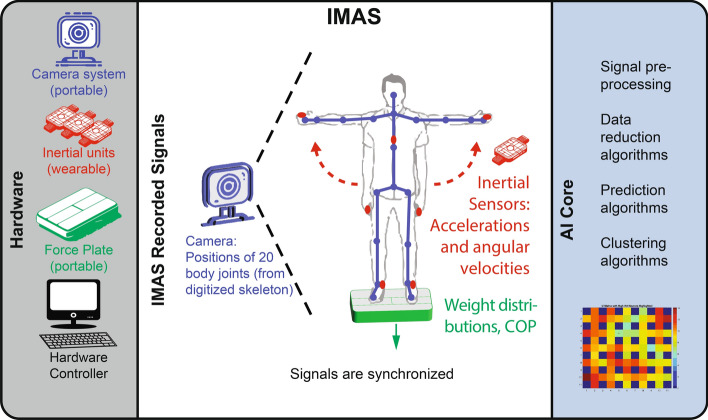
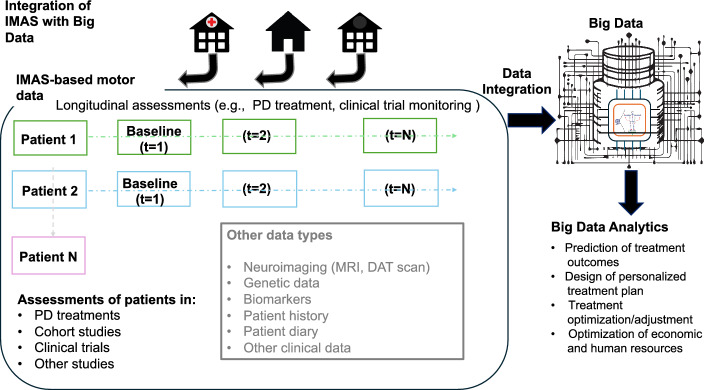
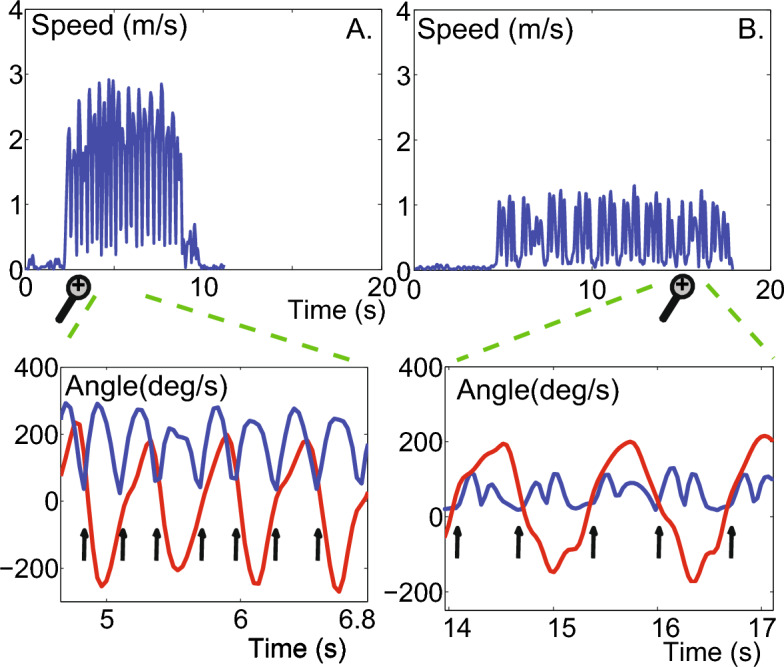
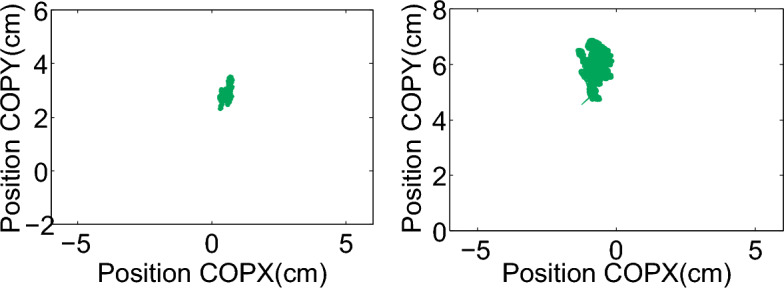
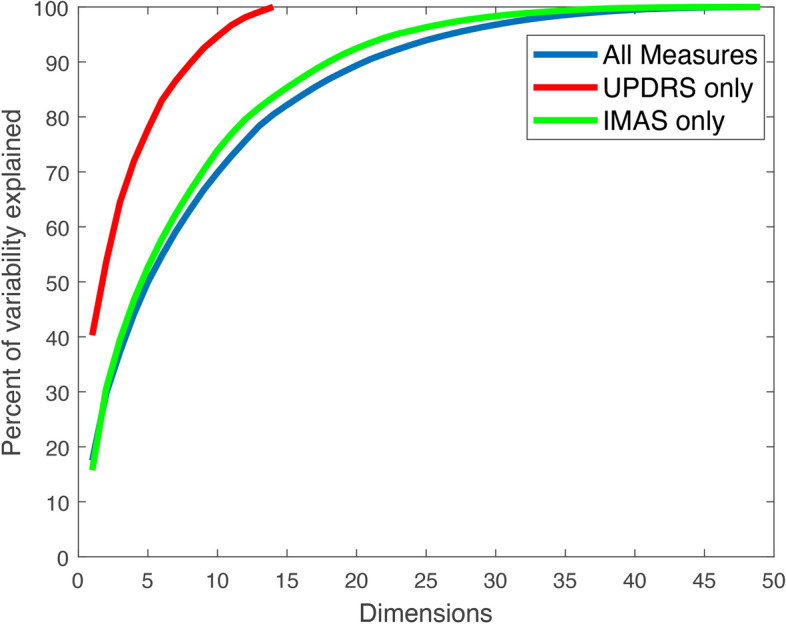
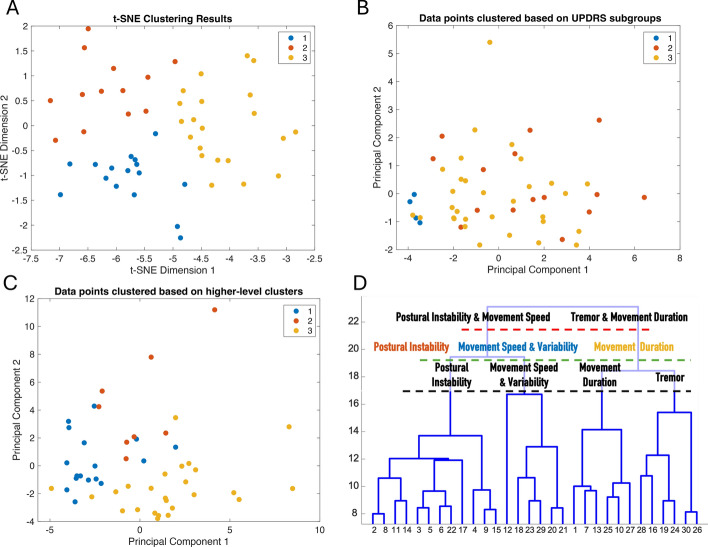
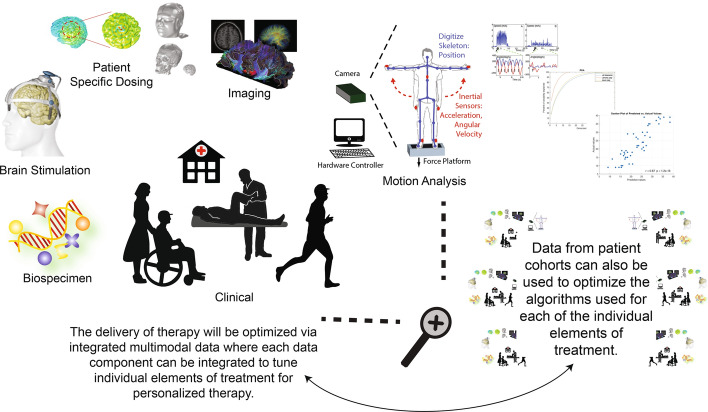
One of the key challenges in Big Data for clinical research and healthcare is how to integrate new sources of data, whose relation to disease processes are often not well understood, with multiple classical clinical measurements that have been used by clinicians for years to describe disease processes and interpret therapeutic outcomes. Without such integration, even the most promising data from emerging technologies may have limited, if any, clinical utility. This paper presents an approach to address this challenge, illustrated through an example in Parkinson's Disease (PD) management. We show how data from various sensing sources can be integrated with traditional clinical measurements used in PD; furthermore, we show how leveraging Big Data frameworks, augmented by Artificial Intelligence (AI) algorithms, can distinctively enrich the data resources available to clinicians. We showcase the potential of this approach in a cohort of 50 PD patients who underwent both evaluations with an Integrated Motion Analysis Suite (IMAS) composed of a battery of multimodal, portable, and wearable sensors and traditional Unified Parkinson's Disease Rating Scale (UPDRS)-III evaluations. Through techniques including Principal Component Analysis (PCA), elastic net regression, and clustering analysis we demonstrate how this combined approach can be used to improve clinical motor assessments and to develop personalized treatments. The scalability of our approach enables systematic data generation and analysis on increasingly larger datasets, confirming the integration potential of IMAS, whose use in PD assessments is validated herein, within Big Data paradigms. Compared to existing approaches, our solution offers a more comprehensive, multi-dimensional view of patient data, enabling deeper clinical insights and greater potential for personalized treatment strategies. Additionally, we show how IMAS can be integrated into established clinical practices, facilitating its adoption in routine care and complementing emerging methods, for instance, non-invasive brain stimulation. Future work will aim to augment our data repositories with additional clinical data, such as imaging and biospecimen data, to further broaden and enhance these foundational methodologies, leveraging the full potential of Big Data and AI.
Keywords: Artificial Intelligence; Big Data; Clustering; Noninvasive brain stimulation; Parkinson’s disease; Precision medicine; Prediction; UPDRS; Wearables.
© The Author(s) 2024.
Conflict of interest statement
Competing interestsTW and LD are officers at Highland Instruments, a medical device company. They have patents pending or issued, personally or as officers in the company, related to imaging, brain stimulation, diagnostics, modeling, and simulation.
Figures
References
-
- Organization WH. Parkinson Disease https://www.who.int/news-room/fact-sheets/detail/parkinson-disease2023
-
- Organization WH. Parkinson disease: a public health approach: technical brief https://www.who.int/publications/i/item/978924005098314 June 2022
Grants and funding
LinkOut - more resources
Full Text Sources