

Perioperative Use of ctDNA to Guide Treatment for Urothelial Carcinoma: The Future is Now
- PMID: 39493820
- PMCID: PMC11530029
- DOI: 10.3233/BLC-230105
Perioperative Use of ctDNA to Guide Treatment for Urothelial Carcinoma: The Future is Now
Abstract
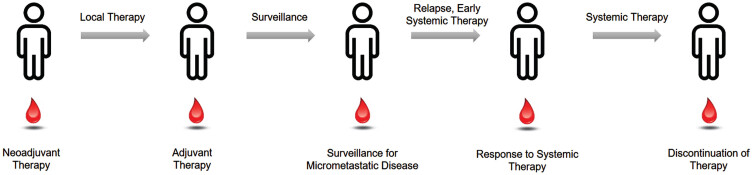
Muscle-invasive bladder cancer represents a potentially curable disease, yet often disease recurs and is ultimately fatal. Outcomes for patients with localized urothelial carcinoma are heterogeneous with some patients cured with surgery alone, deriving no benefit from perioperative systemic therapy, while others are left with residual disease and may benefit from additional therapy. Neoadjuvant chemotherapy increases cure rates but comes with significant toxicity. Recently, adjuvant nivolumab has demonstrated significant improvement in disease free survival (DFS), and overall survival analysis is pending. With more therapies approved for urothelial cancer within the last 5 years than ever before, there is incredible potential to improve clinical outcomes and potentially cure more patients with integrated multimodal therapy. Biomarkers are needed to dichotomize those most likely to benefit from perioperative systemic therapy for residual disease, and de-escalate therapy for those likely to be cured with surgery alone. Ultrasensitive assays for circulating tumor DNA (ctDNA) have emerged as a method to identify patients at high risk of recurrence after definitive therapy and may benefit from escalated therapy, while also identifying those least likely to benefit from systemic therapy. Studies have demonstrated that the presence of ctDNA after surgery is prognostic of disease recurrence across multiple cancer types, including bladder cancer, but questions remain as to the utility of these tests, and whether they can be predictive of benefit of adjuvant therapy. Although these liquid biopsies hold significant promise to transform perioperative treatment, prospective studies are needed to validate their utility as prognostic and predictive biomarkers. To bridge this knowledge gap, contemporary clinical trials are incorporating ctDNA as an integral biomarker to guide therapy for MIBC.
Keywords: Bladder cancer; adjuvant therapy; circulating tumor DNA; ctDNA; muscle-invasive bladder cancer; perioperative therapy.
© 2024 – The authors. Published by IOS Press.
Conflict of interest statement
1.Tyler F. Stewart: Advisory Board/Consulting: Seagen/Astellas, Astrazeneca. Institutional Research Support: GRAIL.2.Heather Chalfin: None3.Nicholas Simon: None4.Alan Tan: Advisory Board/Consulting: BMS, EMD Serono, Gilead, Seagen/Astellas, Merck, Myovant, Natera, Regeneron, Foundation medicine5.Andrea Apolo: None6.Rana R. McKay: Advisory Board/Consulting: AstraZeneca, Aveo, Bayer, Bristol-Myers Squibb, Calithera, Caris, Dendreon, Eli Lilly, Esiai, Exelixis, Janssen, Merck, Myovant, Novartis, Pfizer, Sanofi, SeaGen, Sorrento Therapeutics, Telix, Tempus. Institutional Research Support: AstraZeneca, Artera, Bayer, Bristol-Myers Squibb, Exelixis, Oncternal, Tempus.
Figures

References
-
- Grossman HB, Natale RB, Tangen CM, et al. Neoadjuvant chemotherapy plus cystectomy compared with cystectomy alone for locally advanced bladder cancer. N Engl J Med. 2003;349(9):859–66. - PubMed
-
- Advanced Bladder Cancer Meta-analysis C. Neoadjuvant chemotherapy in invasive bladder cancer: a systematic review and meta-analysis. Lancet. 2003;361(9373):1927–34. - PubMed
-
- Birtle AJ. Updated outcomes of POUT: A phase III randomized trial of peri-operative chemotherapy versus surveillance in upper tract urothelial cancer (UTUC). In: Alison Jane Birtle JDCRJJBJMJJWFCTPRTBABPRCSJ, Rosemere Cancer Centre RPHPUK, Cardiff University CUK, et al. , editors.; 2021; Genitourinary Cancers Symposium: American Society of Clinical Oncology; 2021.
-
- Gupta S, Sonpavde G, Weight CJ, et al. Results from BLASST-1 (Bladder Cancer Signal Seeking Trial) of nivolumab, gemcitabine, and cisplatin in muscle invasive bladder cancer (MIBC) undergoing cystectomy. Journal of Clinical Oncology. 2020;38(6_suppl):439.
-
- Chanza NM, Roumeguere TA, Sideris S, Gil T, Peltier A, Awada A. Avelumab as neoadjuvant therapy in subjects with muscle-invasive urothelial carcinoma (AURA trial). Journal of Clinical Oncology. 2018;36(6_suppl):TPS535–TPS.
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
