

Influence of time to ablation on outcomes among patients with atrial fibrillation with pre-existing heart failure
- PMID: 39493909
- PMCID: PMC11524955
- DOI: 10.1016/j.hroo.2024.07.016
Influence of time to ablation on outcomes among patients with atrial fibrillation with pre-existing heart failure
Abstract
Background: Atrial fibrillation (AF) and heart failure (HF) are cardiac disorders that often coexist.
Objective: This study aimed to investigate how time to ablation could influence the outcomes of AF patients with pre-existing HF.
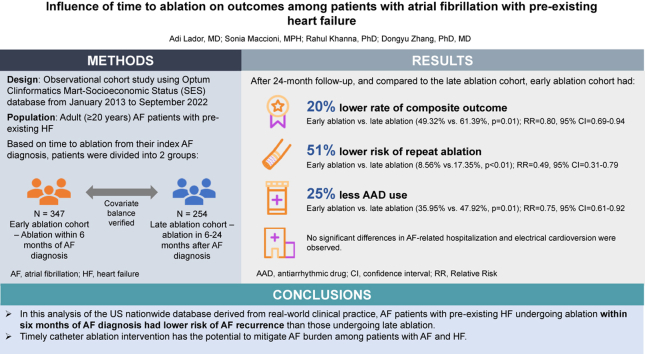
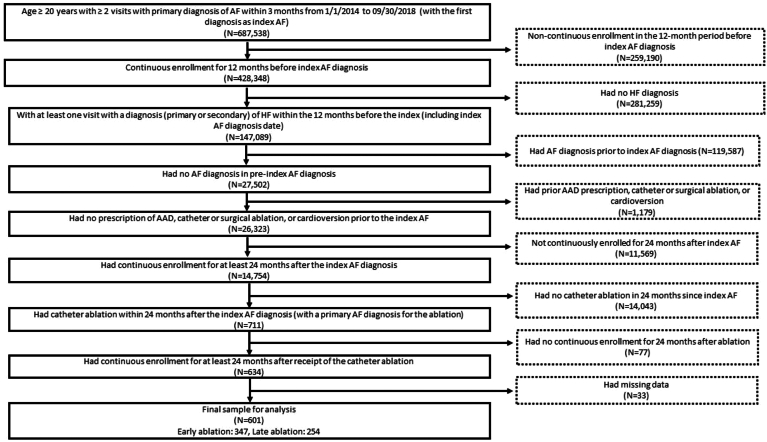
Methods: Using the 2013 to 2022 Optum Clinformatics database, AF patients with pre-existing HF were classified into 2 groups: early ablation (ablation within 6 months of AF diagnosis) and late ablation (ablation in the 6- to 24-month period after AF diagnosis). Outcomes including AF-related hospitalization, electrical cardioversion, repeat ablation, antiarrhythmic drug (AAD) use, and AF recurrence (a composite outcome of the aforementioned events) were assessed in the postblanking 24-month period. Inverse probability of treatment weighted Poisson regression estimated risk ratio (RR) and 95% confidence interval (CI) for each outcome.
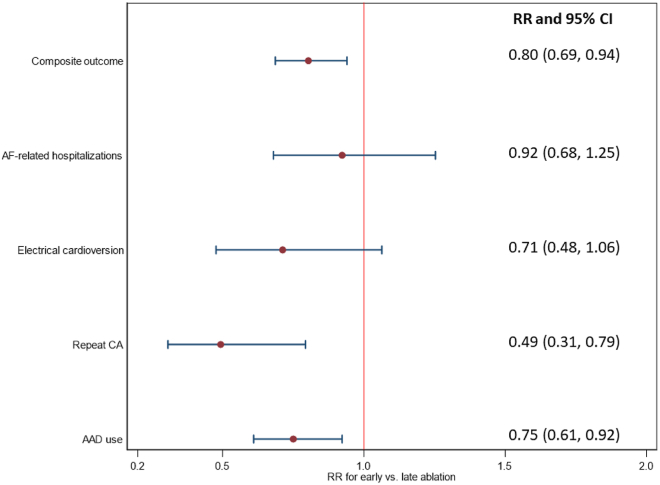
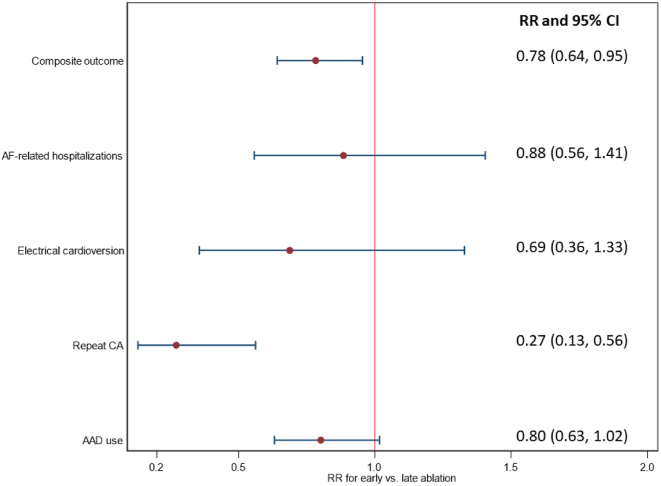
Results: Overall, 601 patients were identified (early ablation: 347; late ablation: 254). In 24 months, the weighted data suggested that patients in the early ablation cohort had significantly lower rate of composite outcome (49.32% vs 61.39%, P = .01), repeat ablation (8.56% vs 17.35%, P < .01), and AAD use (35.95% vs 47.92%, P = .01). Early ablation was associated with a 20%, 51%, and 25% lower risk of composite outcome (RR 0.80, 95% CI 0.69-0.94), repeat ablation (RR 0.49, 95% CI 0.31-0.79), and AAD use (RR 0.75, 95% CI 0.61-0.92), respectively. No significant difference in AF-related hospitalization and electrical cardioversion were observed.
Conclusion: AF patients with pre-existing HF undergoing ablation within 6 months of AF diagnosis have a lower risk of AF recurrence than those undergoing late ablation, which was evidenced by a lower rate of repeat ablation and AAD use.
Keywords: Atrial fibrillation; Cardiology; Catheter ablation; Epidemiology; Heart failure.
© 2024 Heart Rhythm Society. Published by Elsevier Inc.
Figures
References
-
- Moser D.K., Mann D.L. Improving outcomes in heart failure: It's not unusual beyond usual care. Circulation. 2002;105:2810–2812. - PubMed
-
- Braunwald E. Shattuck lecture--cardiovascular medicine at the turn of the millennium: triumphs, concerns, and opportunities. N Engl J Med. 1997;337:1360–1369. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
