

Risk Factors Analysis and Prediction Model Establishment for Carbapenem-Resistant Enterobacteriaceae Colonization: A Retrospective Cohort Study
- PMID: 39494229
- PMCID: PMC11529608
- DOI: 10.2147/IDR.S485915
Risk Factors Analysis and Prediction Model Establishment for Carbapenem-Resistant Enterobacteriaceae Colonization: A Retrospective Cohort Study
Abstract
Purpose: The objective of this study was to identify the risk factors associated with Carbapenem-resistant Enterobacteriaceae (CRE) colonization in intensive care unit (ICU) patients and to develop a predictive risk model for CRE colonization.
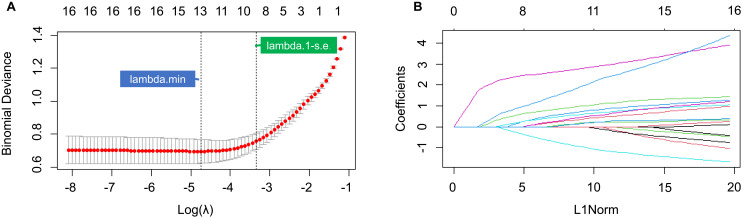
Patients and methods: In this study, 121 ICU patients from Fujian Provincial Hospital were enrolled between January 2021 and July 2022. Based on bacterial culture results from rectal and throat swabs, patients were categorized into two groups: CRE-colonized (n = 18) and non-CRE-colonized (n = 103). To address class imbalance, Synthetic Minority Over-sampling Technique (SMOTE) was applied. Statistical analyses including T-tests, Chi-square tests, and Mann-Whitney U-tests were employed to compare differences between the groups. Feature selection was performed using Lasso regression and Random Forest algorithms. A Logistic regression model was then developed to predict CRE colonization risk, and the results were presented in a nomogram.
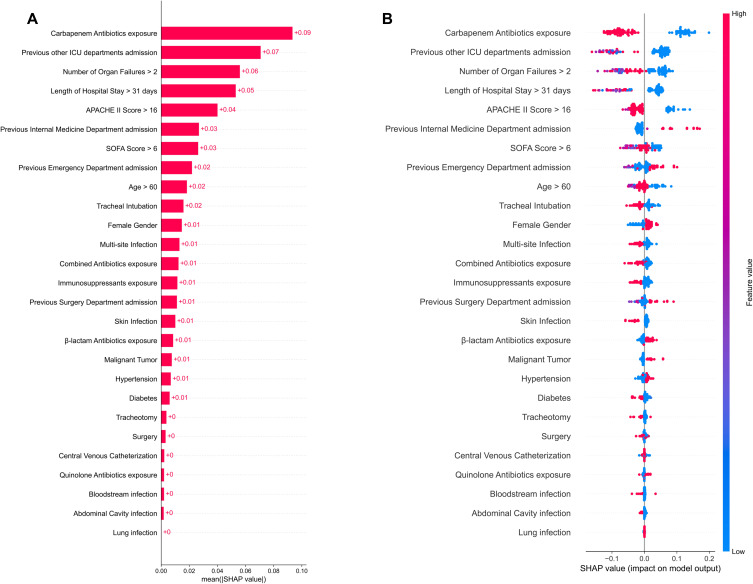
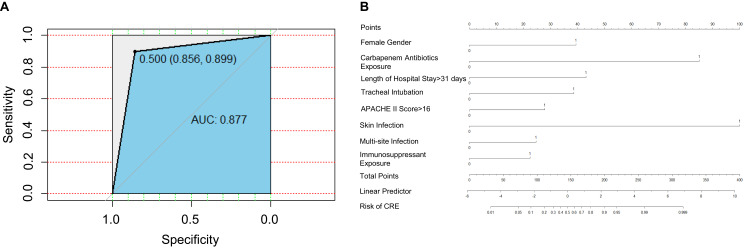
Results: After applying SMOTE, the dataset included 198 CRE-colonized patients and 180 non-CRE-colonized patients, ensuring balanced groups. The two groups were comparable in most clinical characteristics except for diabetes, previous emergency department admission, and abdominal infection. Eight independent risk factors for CRE colonization were identified through Random Forest, Lasso regression, and Logistic regression, including Acute Physiology and Chronic Health Evaluation (APACHE) II score > 16, length of hospital stay > 31 days, female gender, previous carbapenem antibiotic exposure, skin infection, multi-site infection, immunosuppressant exposure, and tracheal intubation. The risk prediction model for CRE colonization demonstrated high accuracy (87.83%), recall rate (89.9%), precision (85.6%), and an AUC value of 0.877. Patients were categorized into low-risk (0-90 points), medium-risk (91-160 points), and high-risk (161-381 points) groups, with corresponding CRE colonization rates of 1.82%, 7.14%, and 58.33%, respectively.
Conclusion: This study identified independent risk factors for CRE colonization and developed a predictive model for assessing the risk of CRE colonization.
Keywords: carbapenem-resistant Enterobacteriaceae; colonization; intensive care unit; risk factors; risk prediction model.
© 2024 Guo et al.
Conflict of interest statement
The authors declare that they have no competing interests in this work.
Figures
Similar articles
-
Carbapenem-resistant Enterobacteriaceae colonization (CRE) and subsequent risk of infection and 90-day mortality in critically ill patients, an observational study.PLoS One. 2017 Oct 12;12(10):e0186195. doi: 10.1371/journal.pone.0186195. eCollection 2017. PLoS One. 2017. PMID: 29023567 Free PMC article.
-
Carbapenem-resistant Enterobacteriaceae colonization and infection in critically ill patients: a retrospective matched cohort comparison with non-carriers.J Hosp Infect. 2016 Sep;94(1):54-9. doi: 10.1016/j.jhin.2016.05.018. Epub 2016 Jun 6. J Hosp Infect. 2016. PMID: 27392978
-
Increased Risk for Carbapenem-Resistant Enterobacteriaceae Colonization in Intensive Care Units after Hospitalization in Emergency Department.Emerg Infect Dis. 2020 Jun;26(6):1156-1163. doi: 10.3201/eid2606.190965. Epub 2020 Jun 17. Emerg Infect Dis. 2020. PMID: 32267827 Free PMC article.
-
Development of a risk prediction model for subsequent infection after colonization with carbapenem-resistant Enterobacterales: a retrospective cohort study.Antimicrob Resist Infect Control. 2024 Apr 24;13(1):46. doi: 10.1186/s13756-024-01394-5. Antimicrob Resist Infect Control. 2024. PMID: 38659068 Free PMC article.
-
[Clinical characteristics of carbapenem-resistant Enterobacteriaceae infection in pediatric liver transplantation recipients].Zhonghua Er Ke Za Zhi. 2020 Aug 2;58(8):640-645. doi: 10.3760/cma.j.cn112140-20200316-00239. Zhonghua Er Ke Za Zhi. 2020. PMID: 32842384 Chinese.
Cited by
-
Clinical characteristics, risk factors and prognosis of Klebsiella pneumoniae infection in patients with different states of immune function: a retrospective study.Front Cell Infect Microbiol. 2025 May 30;15:1539554. doi: 10.3389/fcimb.2025.1539554. eCollection 2025. Front Cell Infect Microbiol. 2025. PMID: 40521023 Free PMC article.
References
-
- China Antimicrobial Resistance Surveillance System. Antimicrobial resistance of bacteria: surveillance report from China antimicrobial resistance surveillance system in 2014-2019[J]. Chin J Infect Control. 2021;20(1):15–31.
LinkOut - more resources
Full Text Sources
