

CAR T Cells and T-Cell Therapies for Cancer: A Translational Science Review
- PMID: 39495525
- PMCID: PMC11808657
- DOI: 10.1001/jama.2024.19462
CAR T Cells and T-Cell Therapies for Cancer: A Translational Science Review
Abstract
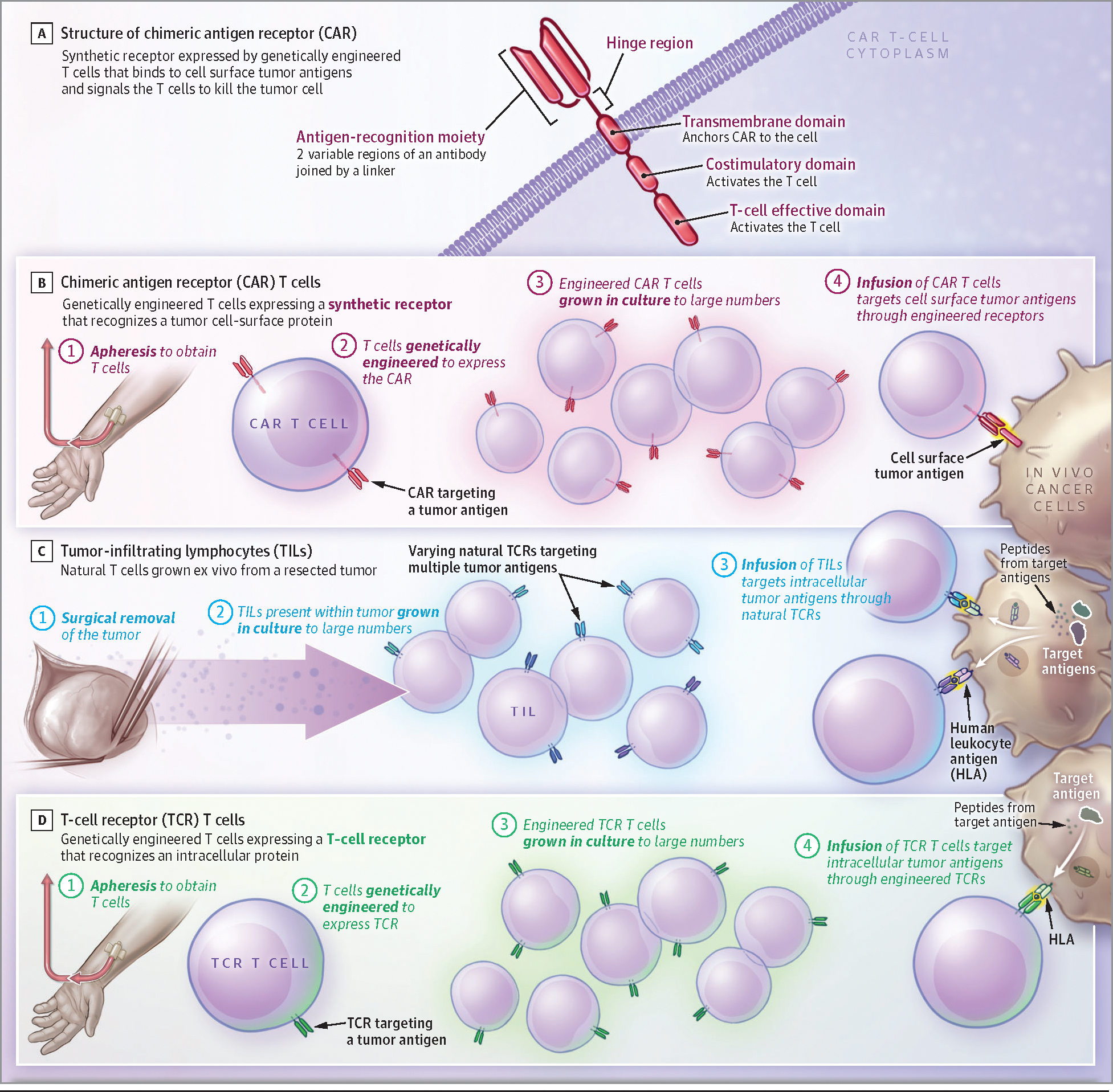
Importance: Chimeric antigen receptor (CAR) T cells are T lymphocytes that are genetically engineered to express a synthetic receptor that recognizes a tumor cell surface antigen and causes the T cell to kill the tumor cell. CAR T treatments improve overall survival for patients with large B-cell lymphoma and progression-free survival for patients with multiple myeloma.
Observations: Six CAR T-cell products are approved by the US Food and Drug Administration (FDA) for 6 hematologic malignancies: B-cell acute lymphoblastic leukemia, large B-cell lymphoma, follicular lymphoma, mantle cell lymphoma, chronic lymphocytic leukemia, and multiple myeloma. Compared with standard chemotherapy followed by stem cell transplant, CAR T cells improved 4-year overall survival in patients with large B-cell lymphoma (54.6% vs 46.0%). Patients with pediatric acute lymphoblastic leukemia achieved durable remission after CAR T-cell therapy. At 3-year follow-up, 48% of patients were alive and relapse free. In people with multiple myeloma treated previously with 1 to 4 types of non-CAR T-cell therapy, CAR T-cell therapy prolonged treatment-free remissions compared with standard treatments (in 1 trial, CAR T-cell therapy was associated with progression-free survival of 13.3 months compared with 4.4 months with standard therapy). CAR T-cell therapy is associated with reversible acute toxicities, such as cytokine release syndrome in approximately 40% to 95% of patients, and neurologic disorders in approximately 15% to 65%. New CAR T-cell therapies in development aim to increase efficacy, decrease adverse effects, and treat other types of cancer. No CAR T-cell therapies are FDA approved for solid tumors, but recently, 2 other T lymphocyte-based treatments gained approvals: 1 for melanoma and 1 for synovial cell sarcoma. Additional cellular therapies have attained responses for certain solid tumors, including pediatric neuroblastoma, synovial cell sarcoma, melanoma, and human papillomavirus-associated cancers. A common adverse effect occurring with these T lymphocyte-based therapies is capillary leak syndrome, which is characterized by fluid retention, pulmonary edema, and kidney dysfunction.
Conclusions and relevance: CAR T-cell therapy is an FDA-approved therapy that has improved progression-free survival for multiple myeloma, improved overall survival for large B-cell lymphoma, and attained high rates of cancer remission for other hematologic malignancies such as acute lymphoblastic leukemia, follicular lymphoma, and mantle cell lymphoma. Recently approved T lymphocyte-based therapies demonstrated the potential for improved outcomes in solid tumor malignancies.
Figures
Comment in
-
Translational Science Reviews-A New JAMA Review.JAMA. 2024 Dec 10;332(22):1888. doi: 10.1001/jama.2024.21146. JAMA. 2024. PMID: 39495501 No abstract available.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
