

Effect of theta burst stimulation on lower extremity motor function improvement and balance recovery in patients with stroke: A systematic review and meta-analysis of randomized controlled trials
- PMID: 39495989
- PMCID: PMC11537599
- DOI: 10.1097/MD.0000000000040098
Effect of theta burst stimulation on lower extremity motor function improvement and balance recovery in patients with stroke: A systematic review and meta-analysis of randomized controlled trials
Abstract
Background: To investigate the therapeutic benefits of theta burst stimulation on lower-limb motor dysfunction and balance recovery in patients with stroke.
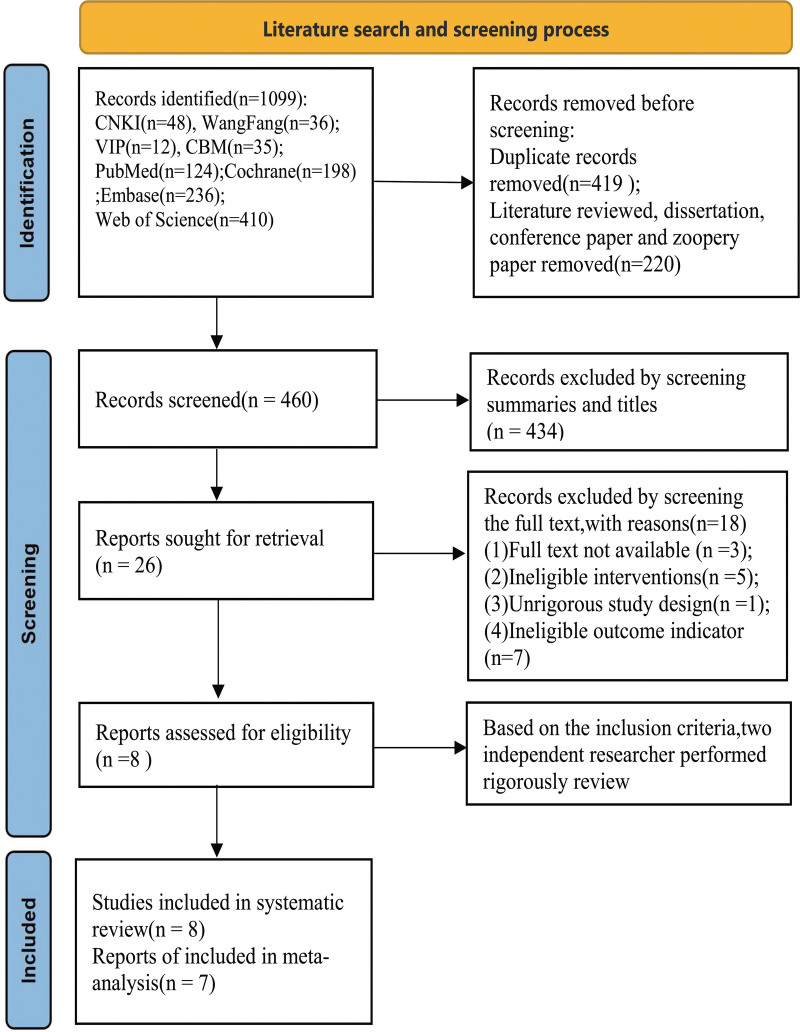
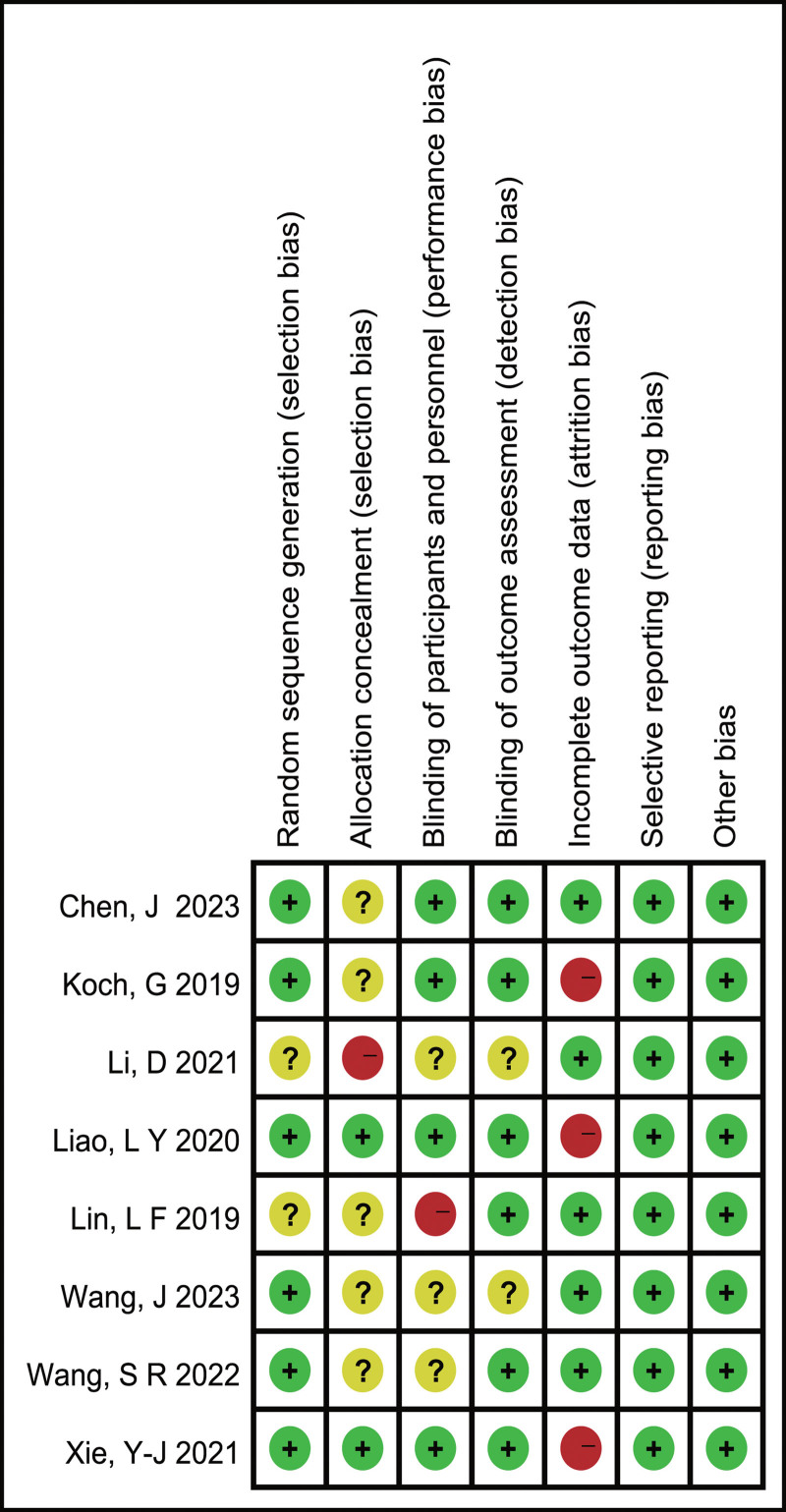
Methods: A literature search was performed across CNKI, CBM, WanFang, VIP, PubMed, Embase, Cochrane Library, and Web of Science until November 2023. The Methodological quality of included studies was assessed by using the Cochrane risk-of-bias tool and the PEDro scale, and the meta-analysis was performed by using RevMan 5.3 software. Two independent researchers screened the literature and extracted basic information on participants, interventions, comparisons, outcomes, and studies.
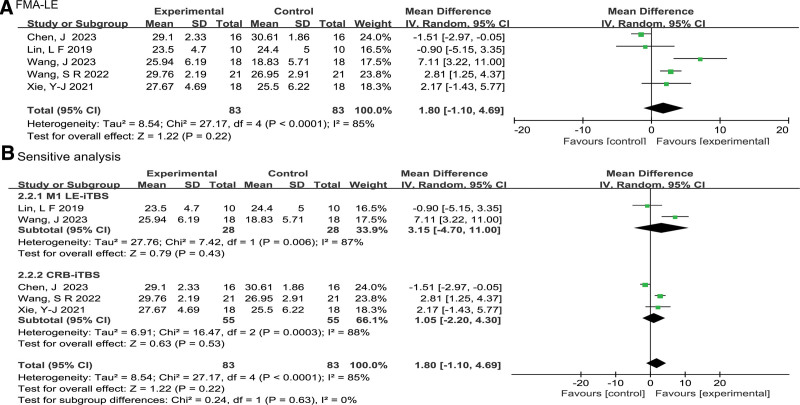
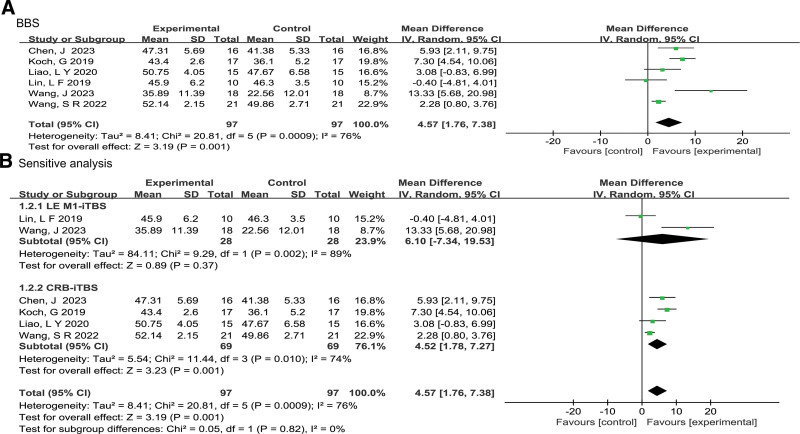
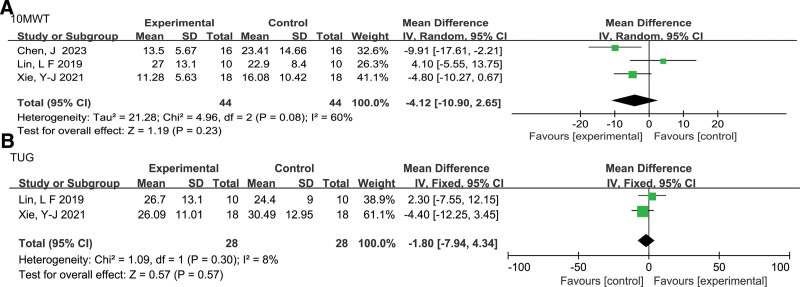
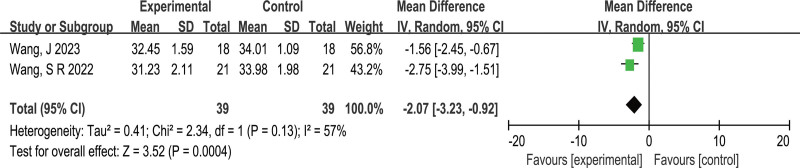
Results: Eight studies, including cTBS and iTBS, with 290 participants meeting the inclusion criteria for this systematic review, and 7 studies including only iTBS with 230 participants were included in this meta-analysis. The methodological quality of the studies included ranged from moderate to high. The results showed iTBS had significantly higher scores on the Berg Balance Scale (BBS) than the control group. (MD = 4.57, 95% CI: 1.76 to 7.38, Z = 3.19, P = .001). Subgroup analysis showed CRB-iTBS markedly improved BBS scores (MD = 4.52, 95% CI: 1.78 to 7.27, Z = 3.23, P = .001), whereas LE M1-iTBS did not exhibit a significant enhancement in BBS scores (MD = 6.10, 95% CI: -7.34 to 19.53, Z = 0.89, P = .37); iTBS showed no significant increase in lower-limb motor function (FMA-LE) (MD = 1.80, 95% CI: -1.10 to 4.69, Z = 1.22, P = .22). Subgroup analysis revealed both CRB-iTBS and LE M1-iTBS interventions were not effective in improving FMA-LE (MD = 3.15, 95% CI: -4.70 to 11.00, Z = .79, P = .43; MD = 1.05, 95% CI: -2.20 to 4.30, Z = .63, P = .53); iTBS significantly reduced the MEP latency (P = .004), but did not show a significant improvement in walking performance (10 MWT), mobility (TUG), or activities of daily living [M(BI)] (P > .05).
Conclusion: Based the current study, iTBS can increase patients' balance function. The CRB-iTBS protocol is more effective than the LE M1-iTBS protocol. Additionally, iTBS may be a promising therapy tending to enhance lower-limb motor function, walking performance, mobility, and activities of daily living.
Copyright © 2024 the Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
The authors have no any conflict of interest to disclose.
Figures

References
-
- Saini V, Guada L, Yavagal DR. Global epidemiology of stroke and access to acute ischemic stroke interventions. Neurology. 2021;97:S6–S16. - PubMed
-
- Pundik S, McCabe J, Skelly M, Tatsuoka C, Daly JJ. Association of spasticity and motor dysfunction in chronic stroke. Ann Phys Rehabil Med. 2019;62:397–402. - PubMed
-
- Yadav T, Bhalerao G, Shyam AK. Factors affecting fear of falls in patients with chronic stroke. Top Stroke Rehabil. 2020;27:33–7. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
