

Association of serum uric acid with all-cause and cardiovascular mortality in cardiovascular disease patients
- PMID: 39496687
- PMCID: PMC11535372
- DOI: 10.1038/s41598-024-76970-1
Association of serum uric acid with all-cause and cardiovascular mortality in cardiovascular disease patients
Abstract
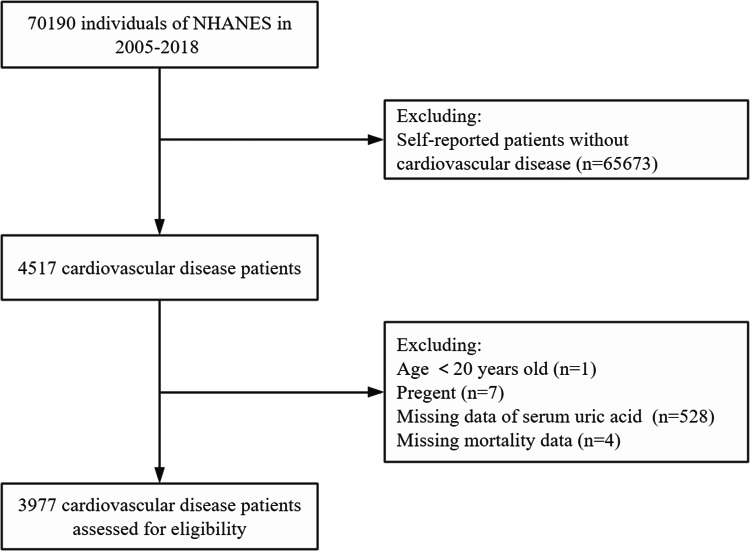
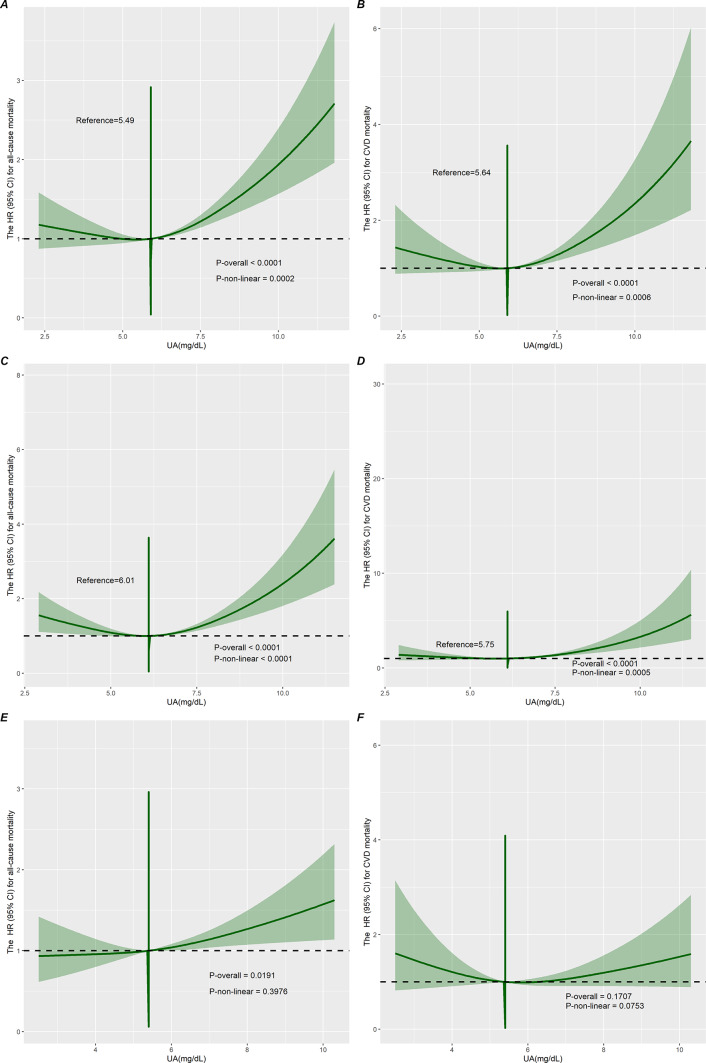
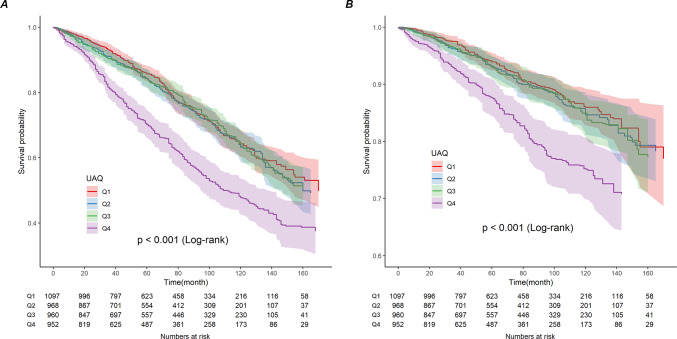
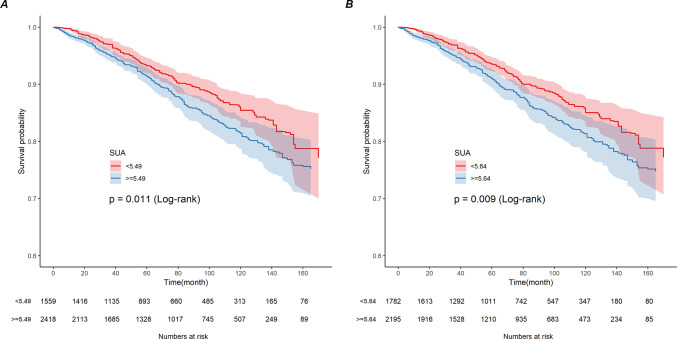
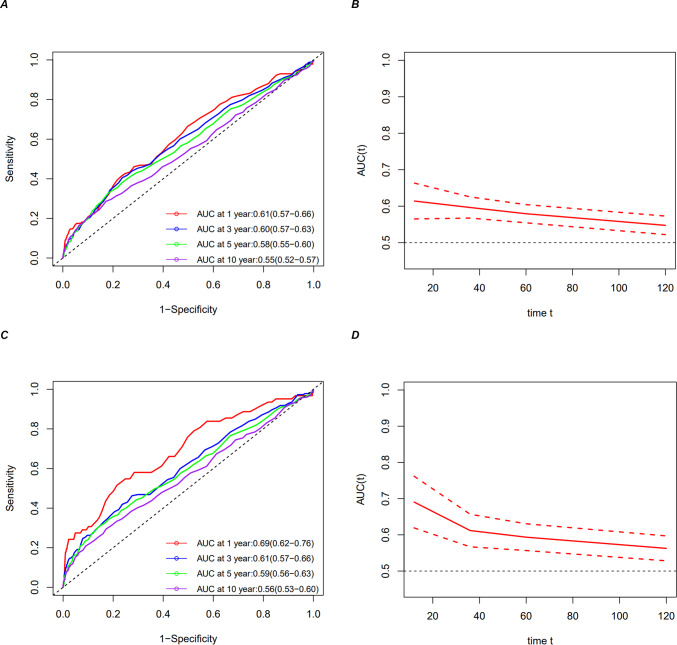
The relationship between serum uric acid (SUA) and mortality in patients with cardiovascular disease (CVD) remains controversial. We aimed to explore the relationship between SUA and all-cause mortality (ACM) and cardiovascular mortality (CVM) in adult patients with CVD. This cohort study included 3977 patients with CVD from the National Health and Nutrition Examination Survey (2005-2018). Death outcomes were determined by linking National Death Index (NDI) records through December 31, 2019. We explored the association of SUA with mortality using weighted Cox proportional hazards regression models, subgroup analysis, Kaplan-Meier survival curves, weighted restricted cubic spline (RCS) models, and weighted threshold effect analysis among patients with CVD. During a median follow-up of 68 months (interquartile range, 34-110 months), 1,360 (34.2%) of the 3,977 patients with cardiovascular disease died, of which 536 (13.5%) died of cardiovascular deaths and 824 (20.7%) died of non-cardiovascular deaths. In a multivariable-adjusted model (Model 3), the risk of ACM (HR 1.38, 95% CI 1.16-1.64) and the risk of CVM (HR 1.39, 95% CI 1.04-1.86) for participants in the SUA Q4 group were significantly higher. In patients with CVD, RCS regression analysis revealed a nonlinear association (p < 0.001 for all nonlinearities) between SUA, ACM, and CVM in the overall population and in men. Subgroup analysis showed a nonlinear association between ACM and CVM with SUA in patients with CVD combined with chronic kidney disease (CKD), with thresholds of 5.49 and 5.64, respectively. Time-dependent ROC curves indicated areas under the curve of 0.61, 0.60, 0.58, and 0.55 for 1-, 3-, 5-, and 10-year survival for ACM and 0.69, 0.61, 0.59, and 0.56 for CVM, respectively. We demonstrate that SUA is an independent prognostic factor for the risk of ACM and CVM in patients with CVD, supporting a U-shaped association between SUA and mortality, with thresholds of 5.49 and 5.64, respectively. In patients with CVD combined with CKD, the association of the ACM and the CVM with SUA remains nonlinear.
Keywords: All-cause mortality; Cardiovascular disease; Cardiovascular mortality; Cohort study; NHANES; Serum uric acid.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
