

Flow cytometry identifies changes in peripheral and intrathecal lymphocyte patterns in CNS autoimmune disorders and primary CNS malignancies
- PMID: 39497174
- PMCID: PMC11536547
- DOI: 10.1186/s12974-024-03269-3
Flow cytometry identifies changes in peripheral and intrathecal lymphocyte patterns in CNS autoimmune disorders and primary CNS malignancies
Abstract
Background: Immune dysregulation is a hallmark of autoimmune diseases of the central nervous system (CNS), characterized by an excessive immune response, and primary CNS tumors (pCNS-tumors) showing a highly immunosuppressive parenchymal microenvironment.
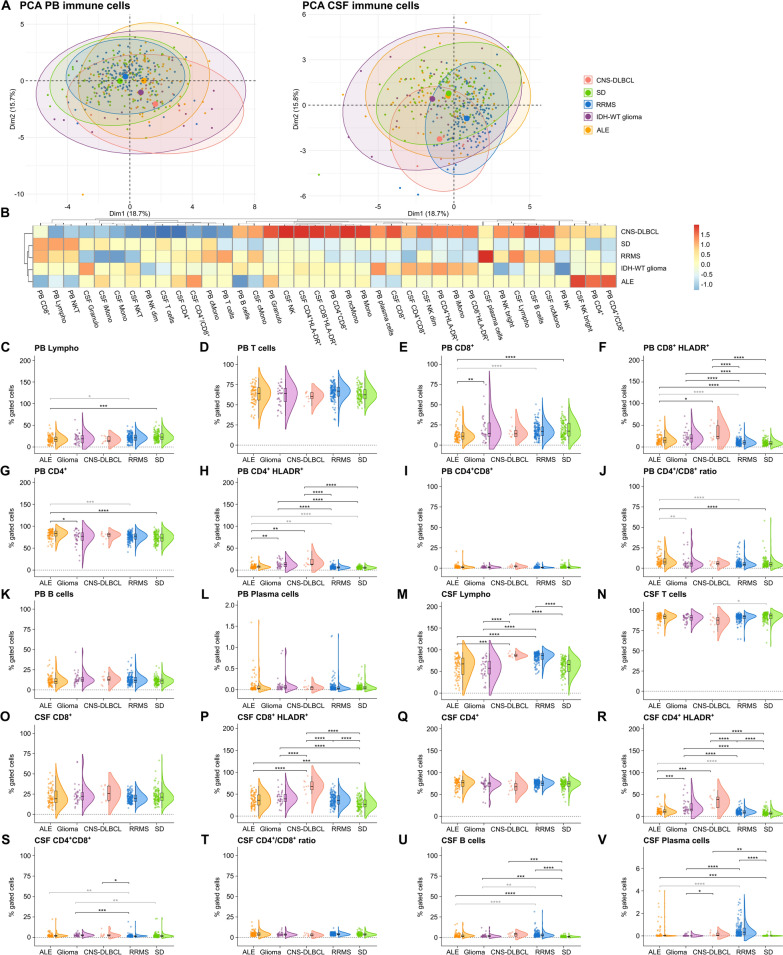
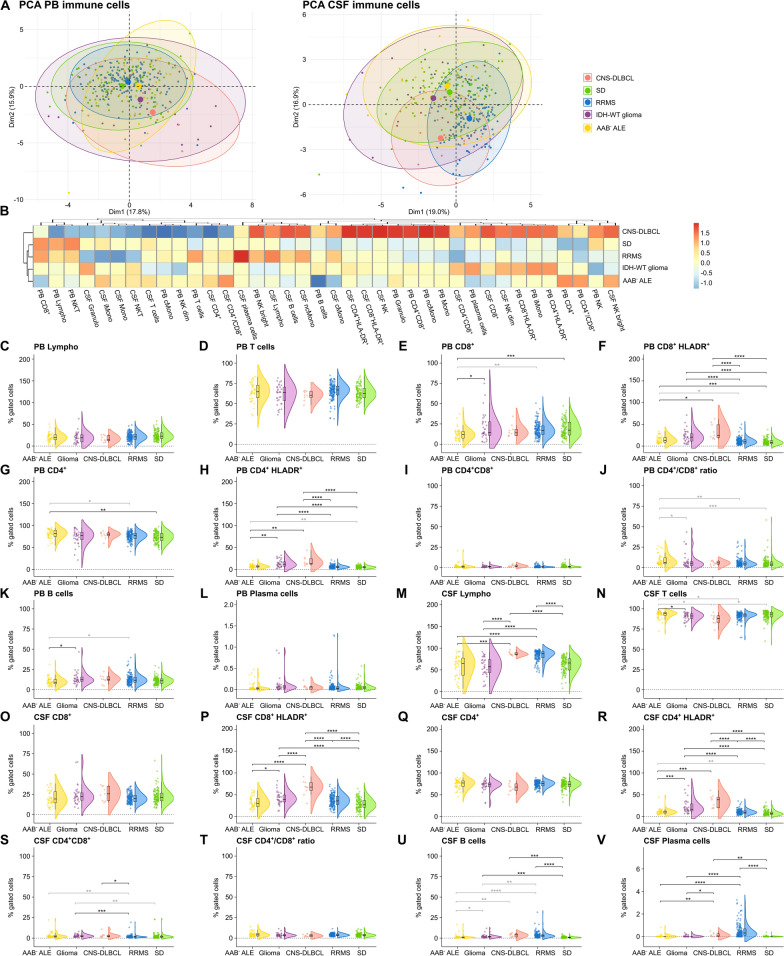
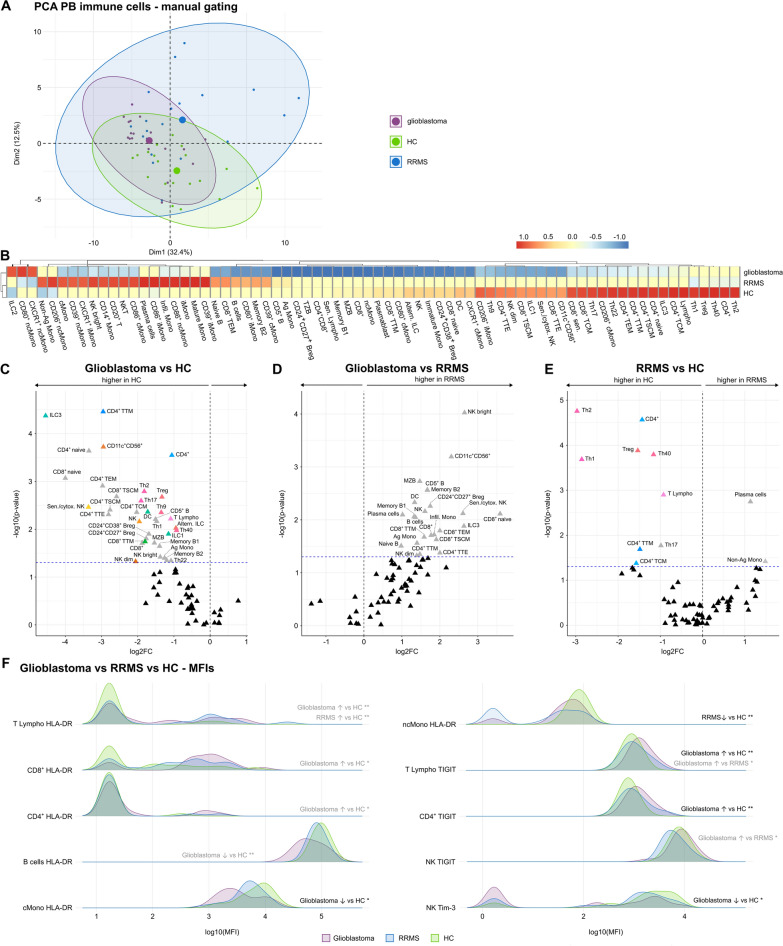
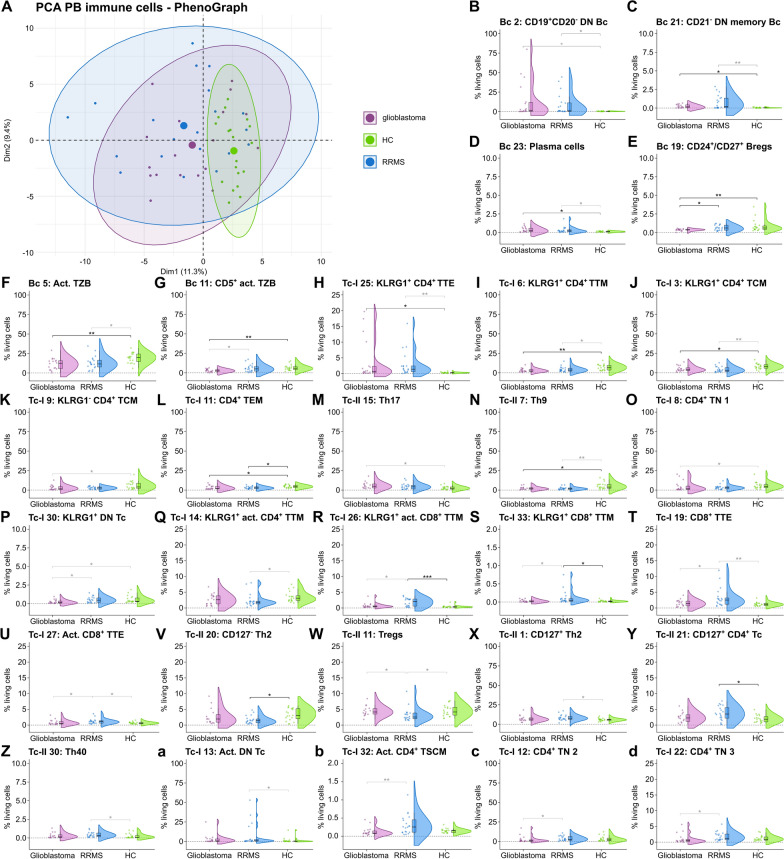
Methods: Aiming to provide novel insights into the pathogenesis of CNS autoimmunity and cerebral tumor immunity, we analyzed the peripheral blood (PB) and cerebrospinal fluid (CSF) of 81 autoimmune limbic encephalitis (ALE), 148 relapsing-remitting multiple sclerosis (RRMS), 33 IDH-wildtype glioma, 9 primary diffuse large B cell lymphoma of the CNS (CNS-DLBCL), and 110 controls by flow cytometry (FC). Additionally, an in-depth immunophenotyping of the PB from an independent cohort of 20 RRMS and 18 IDH-wildtype glioblastoma patients compared to 19 controls was performed by FC combined with unsupervised computational approaches.
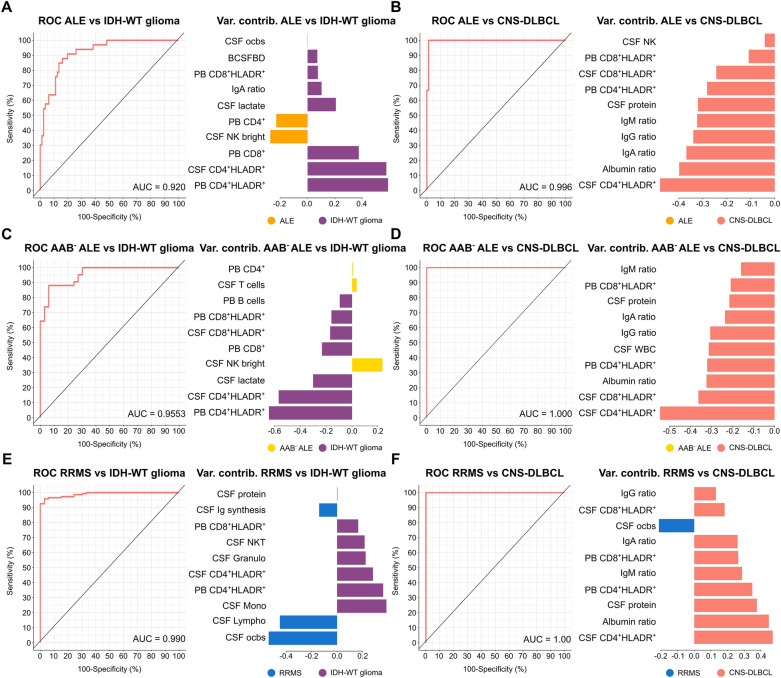
Results: We identified alterations in peripheral and intrathecal adaptive immunity, mainly affecting the T cell (Tc) but also the B cell (Bc) compartment in ALE, RRMS, and pCNS-tumors compared to controls. ALE, RRMS, and pCNS-tumors featured higher expression of the T cell activation marker HLA-DR, which was even more pronounced in pCNS-tumors than in ALE or RRMS. Glioblastoma patients showed signs of T cell exhaustion that were not visible in RRMS patients. In-depth characterization of the PB revealed differences mainly in the T effector and memory compartment between RRMS and glioblastoma patients and similar alterations in the Bc compartment, including atypical Bc, CD19+CD20- double negative Bc, and plasma cells. PB and CSF mFC together with CSF routine parameters could reliably differentiate ALE and RRMS from pCNS-tumors facilitating early diagnosis and treatment.
Conclusions: ALE, RRMS, and pCNS-tumors show distinct but partially overlapping changes mainly in HLA-DR+ Tc, memory Tc, exhausted Tc, and Bc subsets providing insights into disease pathogenesis. Moreover, mFC shows diagnostic potential facilitating early diagnosis and treatment.
Keywords: Autoimmune limbic encephalitis; Glioblastoma; Multidimensional flow cytometry; Primary diffuse large B cell lymphoma of the CNS; Relapsing–remitting multiple sclerosis.
© 2024. The Author(s).
Conflict of interest statement
SK reports funding from the IMF (Innovative medizinische Forschung; I-KO122003) and received research funding from Biogen and honoraria from Eisai, UCB and Jazz Pharma. The remaining authors declare no competing interests related to this study.
Figures
References
MeSH terms
Grants and funding
- 2022-04/Research Committee of the Faculty of Medicine of the Heinrich Heine University Düsseldorf
- KO122003/Innovative Medizinische Forschung
- 01GM1908/German Federal Ministry of Education and Research
- 01GM1908/German Federal Ministry of Education and Research
- 01GM1908/German Federal Ministry of Education and Research
LinkOut - more resources
Full Text Sources
Research Materials
