

Effect of bariatric surgery on the pharmacokinetics of drugs used for attention-deficit hyperactivity disorder-A case series
- PMID: 39497274
- PMCID: PMC11655785
- DOI: 10.1111/bcpt.14099
Effect of bariatric surgery on the pharmacokinetics of drugs used for attention-deficit hyperactivity disorder-A case series
Erratum in
-
Correction to 'Effect of Bariatric Surgery on the Pharmacokinetics of Drugs Used for Attention-Deficit Hyperactivity Disorder-A Case Series'.Basic Clin Pharmacol Toxicol. 2025 Feb;136(2):e14129. doi: 10.1111/bcpt.14129. Basic Clin Pharmacol Toxicol. 2025. PMID: 39821531 Free PMC article. No abstract available.
Abstract
Background: Changes in gastrointestinal physiology following bariatric surgery may affect the pharmacokinetics of drugs. Data on the impact of bariatric surgery on drugs used for attention-deficit/hyperactivity disorder (ADHD) are limited.
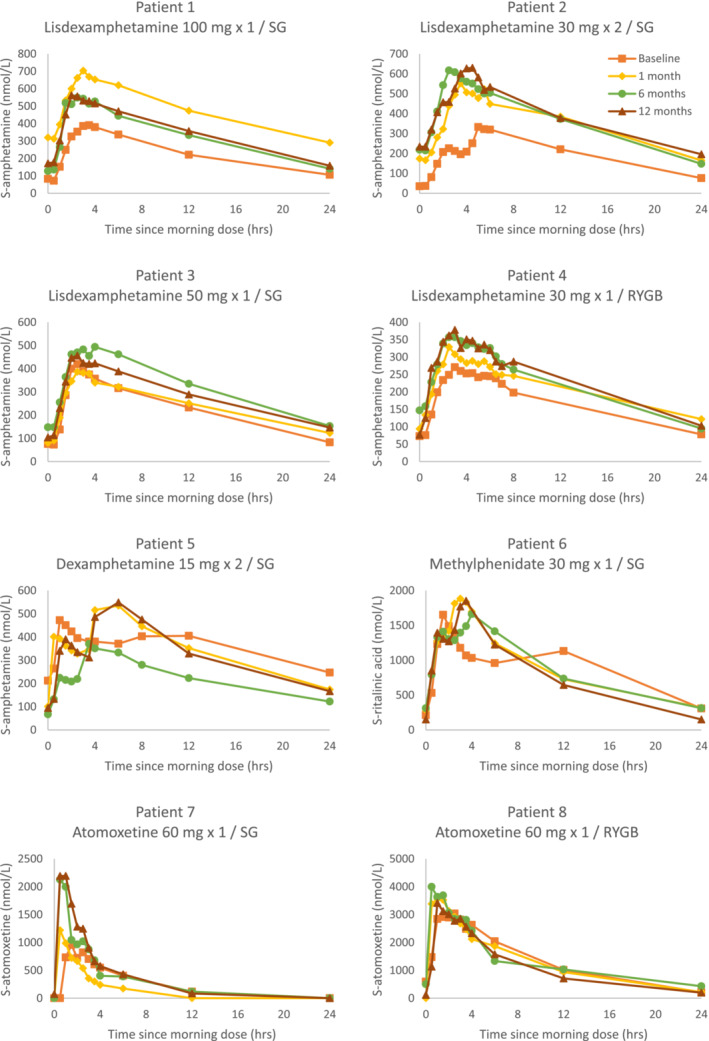
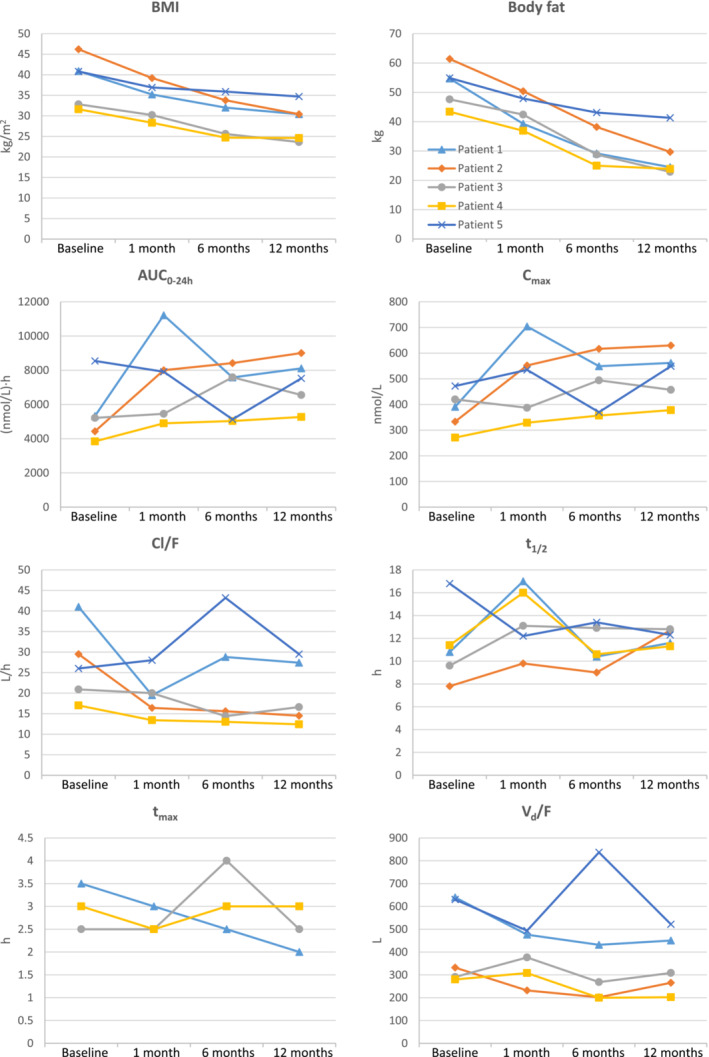
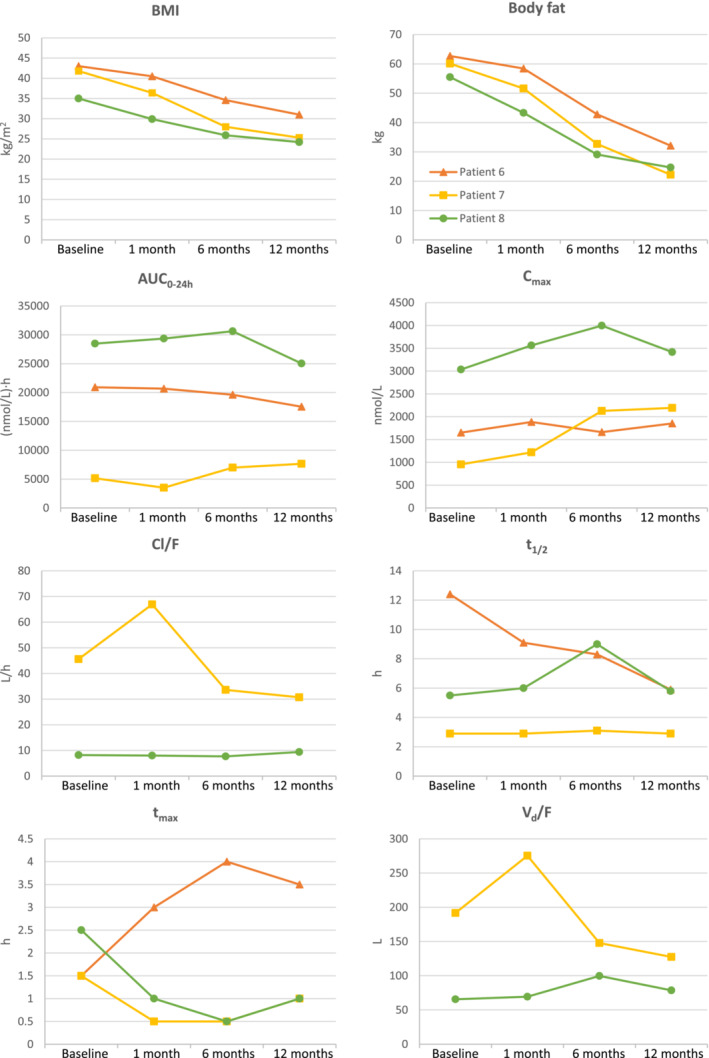
Methods: In patients treated with ADHD medication and undergoing bariatric surgery, serial drug concentrations were measured for 24 h preoperatively and one, six and 12 months postoperatively. Primary outcome was change in area under the concentration-time curve from 0 to 24 h (AUC0-24), with other pharmacokinetic variables as secondary outcomes.
Results: Eight patients treated with lisdexamphetamine (n = 4), dexamphetamine (n = 1), methylphenidate (n = 1) and atomoxetine (n = 2) were included. In total, 409 samples were analysed. Patients underwent sleeve gastrectomy (n = 5) and Roux-en-Y gastric bypass (n = 3). AUC0-24 and Cmax of dexamphetamine increased after surgery in those using the prodrug lisdexamphetamine. There was no clear-cut reduction in tmax postoperatively. For ritalinic acid and atomoxetine, no changes in AUC0-24 were observed, but for atomoxetine, a higher Cmax and a shorter tmax were observed postoperatively.
Conclusion: Bariatric surgery may increase the systemic exposure of dexamphetamine after intake of lisdexamphetamine. Patients using lisdexamphetamine should be followed with regard to adverse drug reactions after bariatric surgery, and, if available, therapeutic drug monitoring should be considered.
Keywords: attention‐deficit hyperactivity disorder; bariatric surgery; case series; dexamphetamine; methylphenidate.
© 2024 The Author(s). Basic & Clinical Pharmacology & Toxicology published by John Wiley & Sons Ltd on behalf of Nordic Association for the Publication of BCPT (former Nordic Pharmacological Society).
Conflict of interest statement
Authors report no competing interests with this work.
Figures
References
-
- World Obesity Federation . World obesity atlas 2024, 2024.
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
