

Development of fully automated models for staging liver fibrosis using non-contrast MRI and artificial intelligence: a retrospective multicenter study
- PMID: 39498462
- PMCID: PMC11532432
- DOI: 10.1016/j.eclinm.2024.102881
Development of fully automated models for staging liver fibrosis using non-contrast MRI and artificial intelligence: a retrospective multicenter study
Abstract
Background: Accurate staging of liver fibrosis (LF) is essential for clinical management in chronic liver disease. While non-contrast MRI (NC-MRI) yields valuable information for liver assessment, its effectiveness in predicting LF remains underexplored. This study aimed to develop and validate artificial intelligence (AI)-powered models utilizing NC-MRI for staging LF.
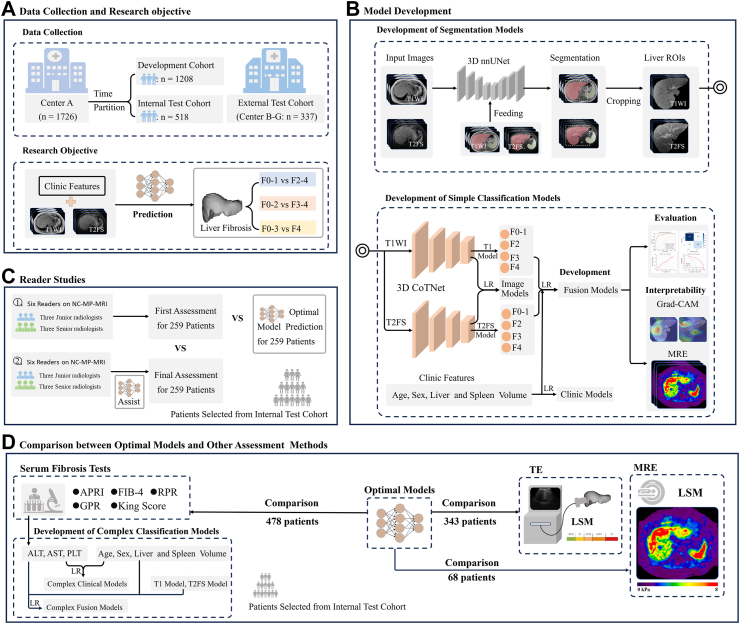
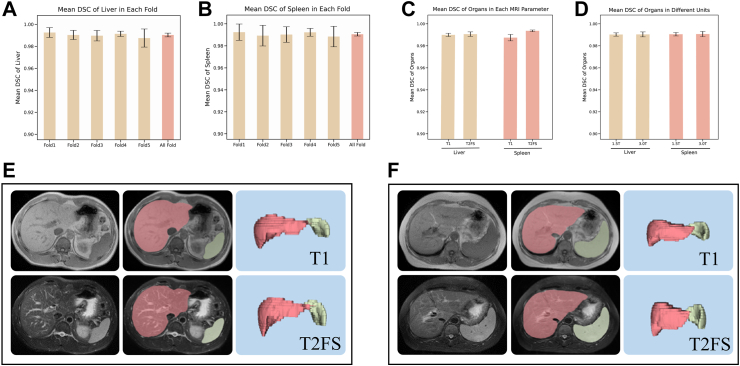
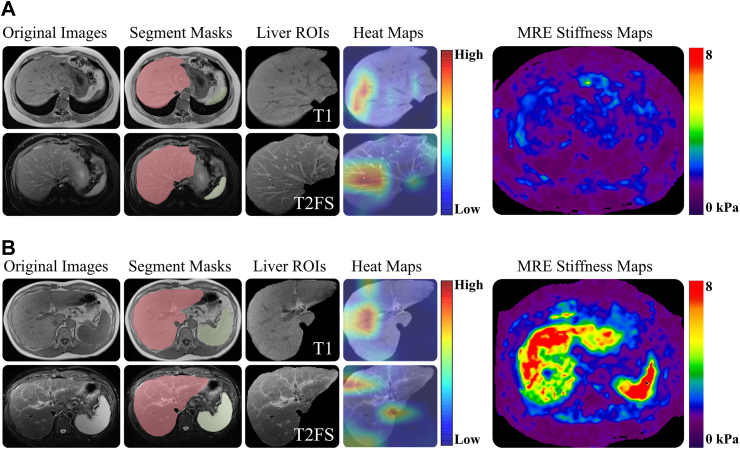
Methods: A total of 1726 patients from Shengjing Hospital of China Medical University, registered between October 2003 and October 2022, were retrospectively collected, and divided into development (n = 1208) and internal test (n = 518) cohorts. An external test cohort consisting of 337 individuals from six centers, registered between June 2015 and November 2022, were also included. All participants underwent NC-MRI (T1-weighted imaging, T1WI; and T2-fat-suppressed imaging, T2FS) and liver biopsies. Two classification models (CMs), named T1 and T2FS, were trained on respective image types using 3D contextual transformer networks and evaluated on both test cohorts. Additionally, three CMs-Clinic, Image, and Fusion-were developed using clinical features, T1 and T2FS scores, and their integration via logistic regression. Classification effectiveness of CMs was assessed using the area under the receiver operating characteristic curve (AUC). A comparison was conducted between the optimal models (OMs) with highest AUC and other methods (transient elastography, five serum biomarkers, and six radiologists).
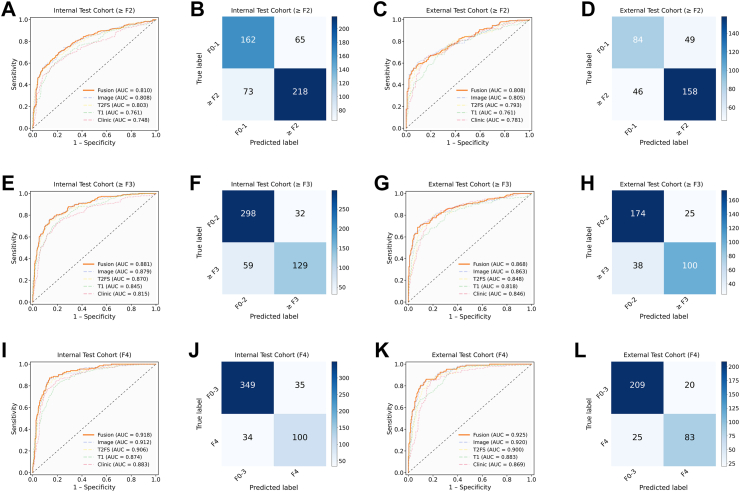
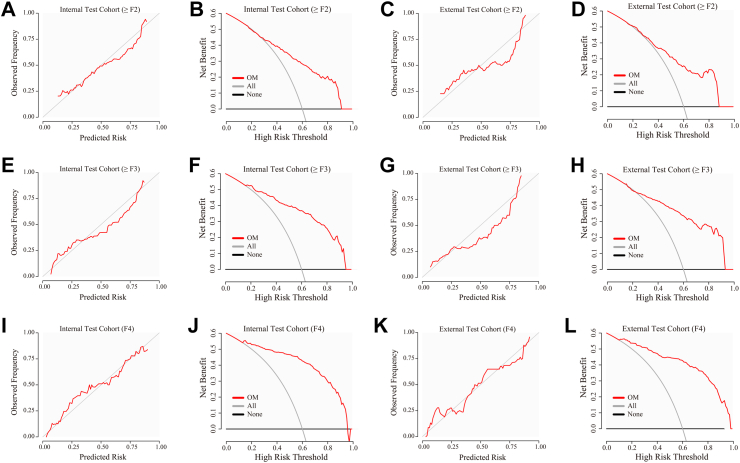
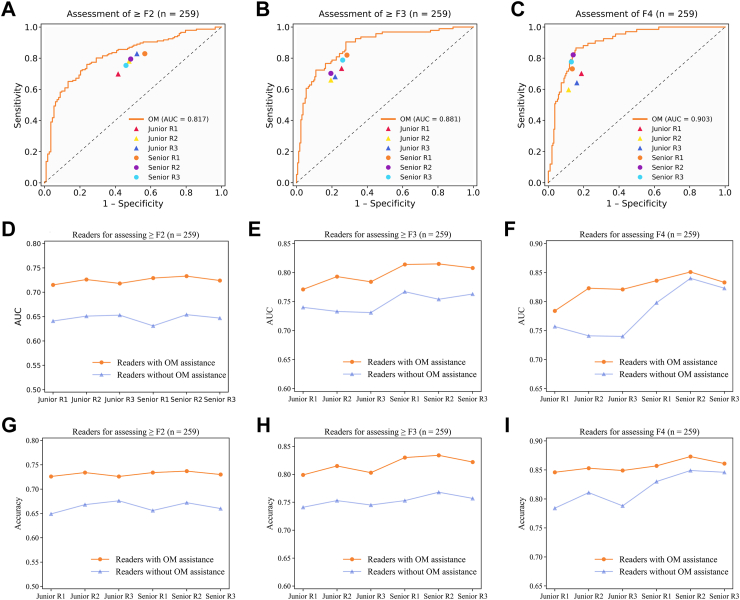
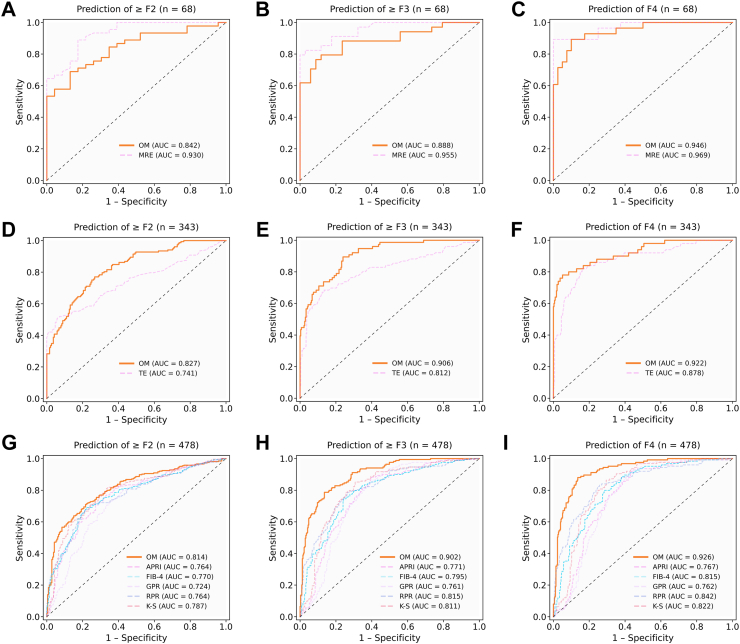
Findings: Fusion models (i.e., OM) yielded the highest AUC among the CMs, achieving AUCs of 0.810 for significant fibrosis, 0.881 for advanced fibrosis, and 0.918 for cirrhosis in the internal test cohort, and 0.808, 0.868, and 0.925, respectively, in the external test cohort. The OMs demonstrated superior performance in AUC, significantly surpassing transient elastography (only for staging ≥ F2 and ≥ F3 grades), serum biomarkers, and three junior radiologists for staging LF. Radiologists, with the aid of the OMs, can achieve a higher AUC in LF assessment.
Interpretation: AI-powered models utilizing NC-MRI, including T1WI and T2FS, accurately stage LF.
Funding: National Natural Science Foundation of China (No. 82071885); General Program of the Liaoning Provincial Department of Education (LJKMZ20221160); Liaoning Province Science and Technology Joint Plan (2023JH2/101700127); the Leading Young Talent Program of Xingliao Yingcai in Liaoning Province (XLYC2203037).
Keywords: Artificial intelligence; Liver fibrosis; Multicenter study; Non-contrast MRI.
© 2024 The Author(s).
Conflict of interest statement
We declare no competing interests related to this study.
Figures
References
LinkOut - more resources
Full Text Sources
Miscellaneous
