

CBCT-based online adaptive radiotherapy of the prostate bed: first clinical experience and comparison to nonadaptive conventional IGRT
- PMID: 39499306
- PMCID: PMC12283463
- DOI: 10.1007/s00066-024-02323-6
CBCT-based online adaptive radiotherapy of the prostate bed: first clinical experience and comparison to nonadaptive conventional IGRT
Abstract
Purpose: Conventional image-guided radiotherapy (IGRT) of the prostate bed is challenged by the varying anatomy due to dynamic changes of surrounding organs such as the bladder and rectum. This leads to changed dose coverage of target and surrounding tissue. The novel online adaptive radiotherapy (oART) aims to improve target coverage as well as reduce dose exposure to surrounding healthy tissues by daily reoptimization of treatment plans. Here we set out to quantify the resulting changes of this adaptation for patients and treatment team.
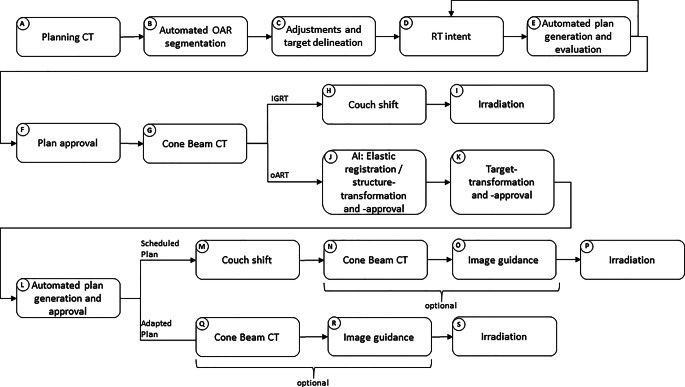
Methods: A total of 198 fractions of radiotherapy of the prostate bed (6 patients) were treated using oART with the Ethos accelerator (Varian Medical Systems, Palo Alto, CA, USA). For each fraction, volumes and several dose-volume parameters of target volumes and organs at risk were recorded for the scheduled plan (initial plan, recalculated based on daily cone beam computed tomography [CBCT]), the adapted plan, and the verification plan, which is the dose distribution of the applied plan recalculated on the closing CBCT after the adaptation process. Clinical acceptability for all plans was determined using given dose-volume parameters of target volumes. Additionally, the time needed for the adaptation process was registered and compared to the time required for the daily treatment of five conventional IGRT patients.
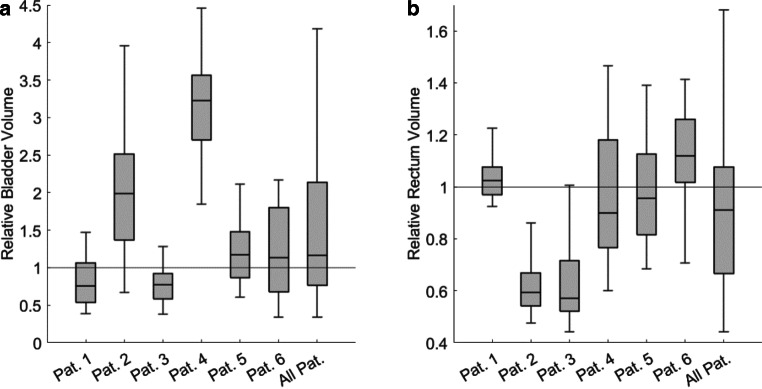
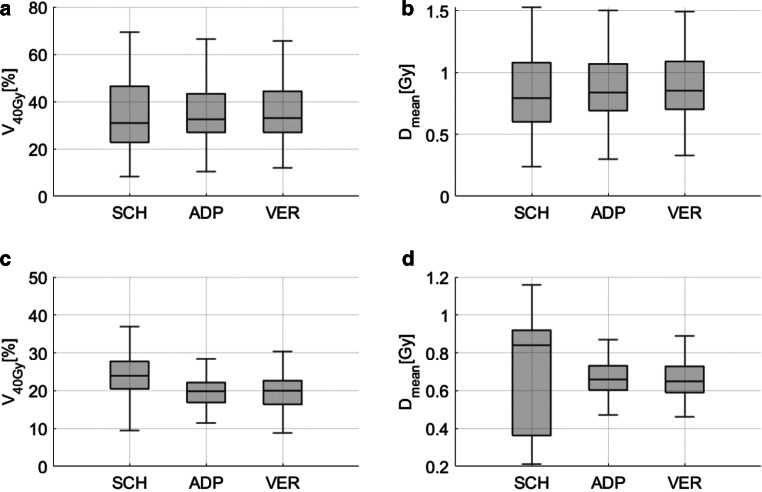
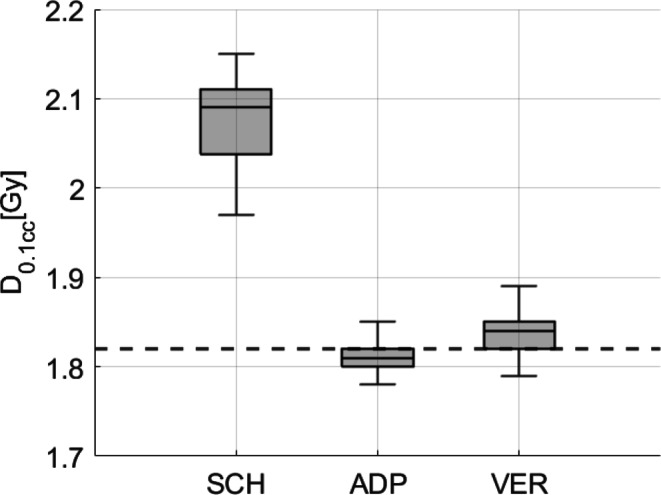
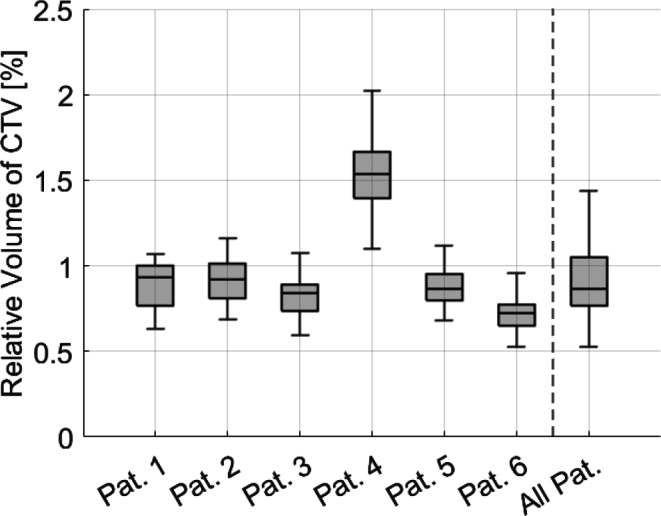
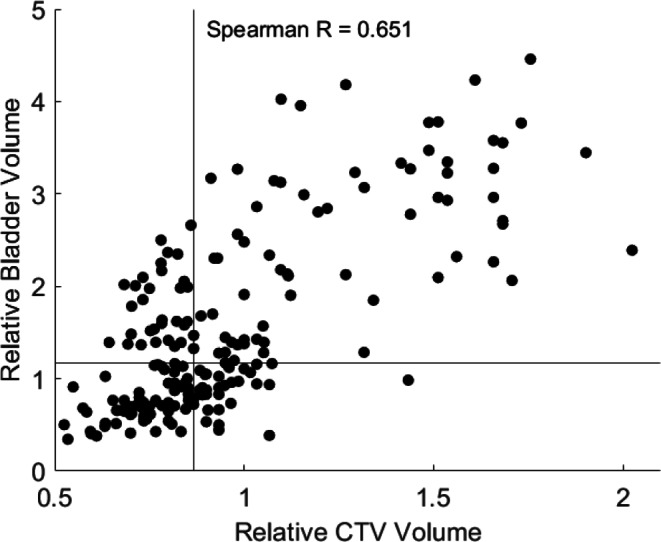
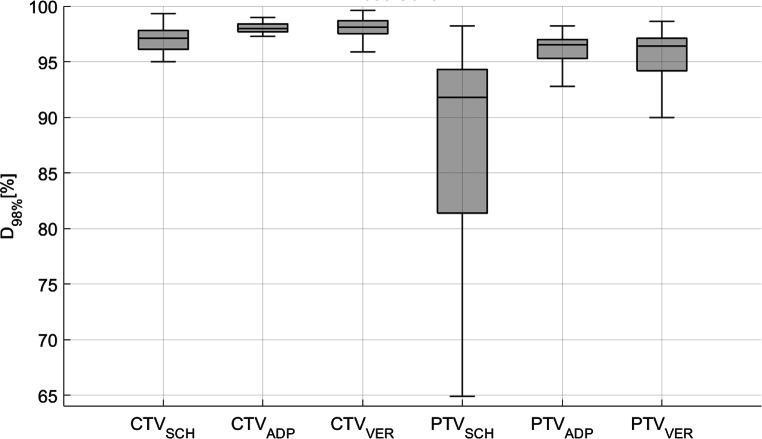
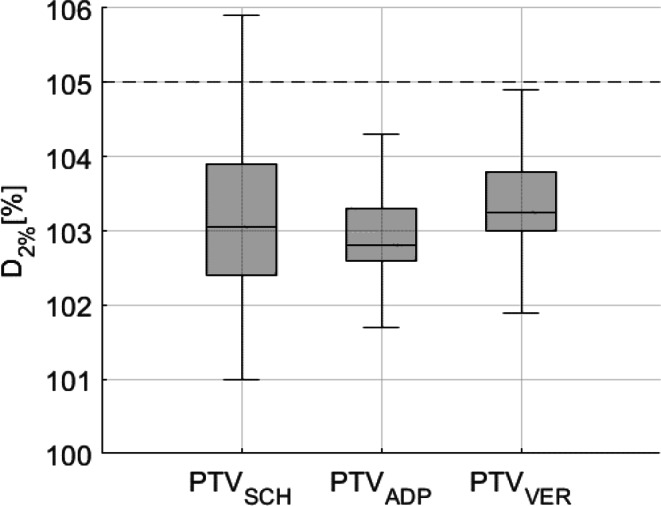
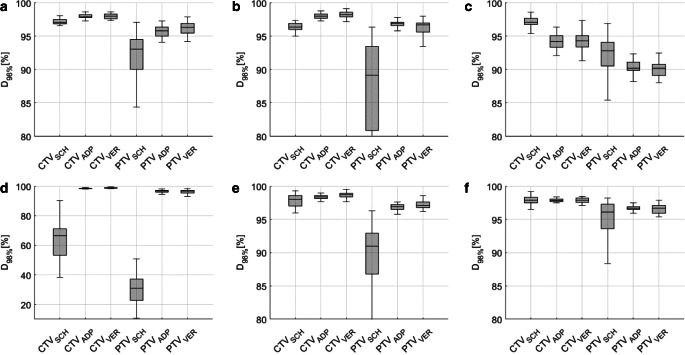
Results: Volumes of target and organs at risk (OAR) exhibited broad variation from day to day. The differences in dose coverage D98% of the clinical target volume (CTV) were significant through adaptation (p < 0.0001; median D98% 97.1-98.0%) and further after verification CBCT (p < 0.001; median D98% 98.1%). Similarly, differences in D98% of the planning target volume (PTV) were significant with adaptation (p < 0.0001; median D98% 91.8-96.5%) and after verification CBCT (p < 0.001; median D98% 96.4%) with decreasing interquartile ranges (IQR). Dose to OAR varied extensively and did not show a consistent benefit from oART but decreased in IQR. Clinical acceptability increased significantly from 19.2% for scheduled plans to 76.8% for adapted plans and decreased to 70.7% for verification plans. The scheduled plan was never chosen for treatment. The median time needed for oART was 25 min compared to 8 min for IGRT.
Conclusion: Target dose coverage was significantly improved using oART. IQR decreased for target coverage as well as OAR doses indicating higher repeatability of dose delivery using oART. Differences in doses after verification CBCT for targets as well as OAR were significant compared to adapted plans but did not offset the overall dosimetric gain of oART. The median time required is three times higher for oART compared to IGRT.
Keywords: Image-guided radiotherapy; Intensity-modulated radiotherapy; Organs at risk; Prostate cancer; Target coverage.
© 2024. The Author(s).
Conflict of interest statement
Conflict of interest: J. Fischer, L. A. Fischer, J. Bensberg, N. Bojko, M. Bouabdallaoui, J. Frohn, P. Hüttenrauch, K. Tegeler, D. Wagner, A. Wenzel, D. Schmitt, M. Guhlich, M. Leu, R. El Shafie, G. Stamm, A.-F. Schilling, L. H. Dröge and S. Rieken declare that they have no competing interests.
Figures
Similar articles
-
CBCT-based online adaptive radiotherapy of the bladder - geometrical and dosimetrical considerations compared to conventional IGRT.Radiat Oncol. 2025 Aug 14;20(1):128. doi: 10.1186/s13014-025-02710-y. Radiat Oncol. 2025. PMID: 40813674 Free PMC article.
-
AI-driven online adaptive radiotherapy in prostate cancer treatment: considerations on activity time and dosimetric benefits.Radiat Oncol. 2025 Jul 25;20(1):116. doi: 10.1186/s13014-025-02697-6. Radiat Oncol. 2025. PMID: 40713724 Free PMC article.
-
Evaluation of the efficacy of automated machine learning enhanced planning system and a comparative analysis with manual planning system.J Cancer Res Ther. 2025 Apr 1;21(3):593-601. doi: 10.4103/jcrt.jcrt_1373_24. Epub 2025 Jul 5. J Cancer Res Ther. 2025. PMID: 40616541
-
From CBCT to MR-Linac in Image-Guided Prostate Cancer Radiotherapy Towards Treatment Personalization.Curr Oncol. 2025 May 22;32(6):291. doi: 10.3390/curroncol32060291. Curr Oncol. 2025. PMID: 40558234 Free PMC article. Review.
-
Adaptive radiotherapy strategies for pelvic tumors - a systematic review of clinical implementations.Acta Oncol. 2016 Aug;55(8):943-58. doi: 10.3109/0284186X.2016.1156738. Epub 2016 Apr 8. Acta Oncol. 2016. PMID: 27055486
Cited by
-
Intra-adaptational changes in online adaptive radiotherapy: from the ideal to the real dose.Strahlenther Onkol. 2025 Jul 15. doi: 10.1007/s00066-025-02425-9. Online ahead of print. Strahlenther Onkol. 2025. PMID: 40663147
References
-
- Yan D, Vicini F, Wong J, Martinez A (1997) Adaptive radiation therapy. Phys Med Biol 42:123. 10.1088/0031-9155/42/1/008 - PubMed
-
- van Herk M, Remeijer P, Rasch C, Lebesque JV (2000) The probability of correct target dosage: dose-population histograms for deriving treatment margins in radiotherapy. Int J Radiat Oncol Biol Phys 47:1121–1135. 10.1016/S0360-3016(00)00518-6 - PubMed
-
- Morgan-Fletcher SL (2001) Prescribing, recording and reporting photon beam therapy (supplement to ICRU report 50), ICRU report 62. ICRU, pp. ix+52, 1999 (ICRU Bethesda, MD) ISBN 0‑913394-61‑0. Br J Radiol 74:294–294. 10.1259/bjr.74.879.740294
-
- Sonke J‑J, Aznar M, Rasch C (2019) Adaptive radiotherapy for anatomical changes. Semin Radiat Oncol 29:245–257. 10.1016/j.semradonc.2019.02.007 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
