

Pressure-Mediated Biofeedback With Pelvic Floor Muscle Training for Urinary Incontinence: A Randomized Clinical Trial
- PMID: 39499517
- PMCID: PMC11539013
- DOI: 10.1001/jamanetworkopen.2024.42925
Pressure-Mediated Biofeedback With Pelvic Floor Muscle Training for Urinary Incontinence: A Randomized Clinical Trial
Abstract
Importance: Supervised pelvic floor muscle training (PFMT) has been recommended as the first-line treatment for women with stress urinary incontinence (SUI), but more evidence on whether adjunctive methods would provide additional benefits is needed.
Objective: To compare the efficacy of PFMT with or without a home-based pressure-mediated biofeedback (BF) device.
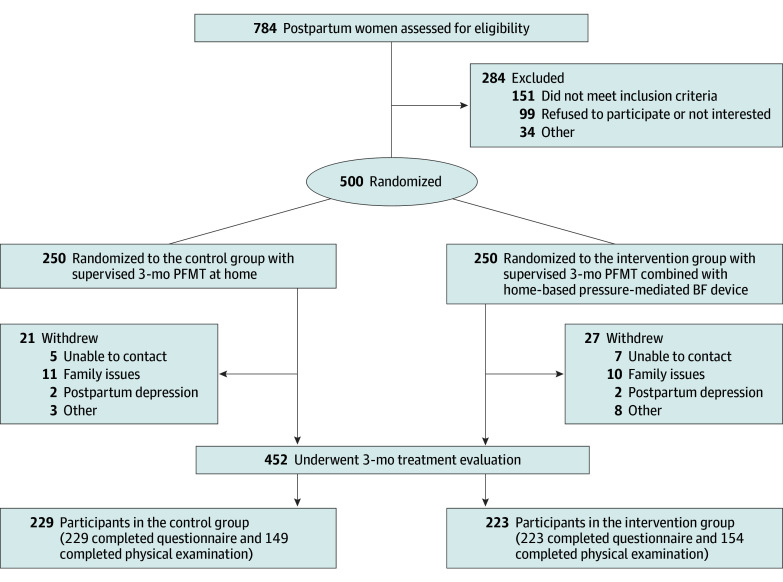
Design, setting, and participants: This multicenter assessor-blinded randomized clinical trial was conducted in the obstetric clinics of 5 participating tertiary hospitals in China. Participants included eligible women with new-onset postpartum SUI who were enrolled from March 28, 2022, to October 13, 2023.
Intervention: All participants received 3 months of supervised PFMT and were randomized to either the intervention (PFMT with a home-based pressure-mediated BF device) or the control group (home-based PFMT).
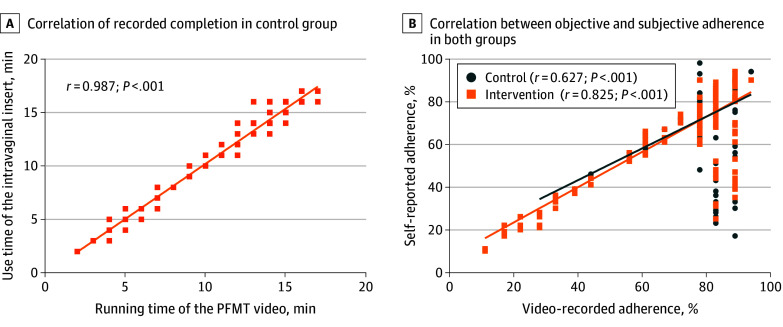
Main outcome and measures: The primary outcome was the severity of urinary incontinence evaluated by the International Consultation on Incontinence Questionnaire-Urinary Incontinence Short Form after 3 months of supervised PFMT. The secondary outcomes included the cure and improvement rates, PFM strength, quality of life, self-efficacy, and adherence.
Results: A total of 452 participants (median age, 34 [IQR, 31-36] years; median body mass index [calculated as the weight in kilograms divided by the height in square meters], 23.71 [IQR, 21.37-25.97]; median time since delivery, 50 [IQR, 43-61] days) were included in the analysis, with 223 in the intervention group and 229 in the control group. Compared with the control group, the intervention group achieved a significantly greater reduction in incontinence severity (median, 3.00 [IQR, 1.00-6.00] vs 2.00 [IQR, 0-4.00] points; z = -3.05; P = .002), significantly increased cure rate (45 of 223 [20.2%] vs 20 of 229 [8.7%]; z = 12.02; P = .001) and improvement (132 of 223 [59.2%] vs 102 of 229 [44.5%]; z = 9.71; P = .002), significantly greater pelvic floor muscle strength (median, 26.00 [IQR, 17.00-38.00] vs 21.00 [IQR, 13.50-33.50] cm H2O; z = -2.28; P = .02), and a significantly greater correlation between subjective and objective adherence (r = 0.825 vs r = 0.627).
Conclusion and relevance: In this randomized clinical trial, the efficacy of pressure-mediated BF combined with PFMT was superior to that of PFMT alone. These findings support the use of pressure-mediated BF devices for improving treatment outcomes for patients with SUI.
Trial registration: ClinicalTrials.gov Identifier: NCT05115864.
Conflict of interest statement
Figures
Similar articles
-
Pelvic Floor Muscle Training for Urinary Incontinence with or without Biofeedback or Electrostimulation in Women: A Systematic Review.Int J Environ Res Public Health. 2022 Feb 27;19(5):2789. doi: 10.3390/ijerph19052789. Int J Environ Res Public Health. 2022. PMID: 35270480 Free PMC article.
-
Conservative interventions for treating urinary incontinence in women: an Overview of Cochrane systematic reviews.Cochrane Database Syst Rev. 2022 Sep 2;9(9):CD012337. doi: 10.1002/14651858.CD012337.pub2. Cochrane Database Syst Rev. 2022. PMID: 36053030 Free PMC article.
-
Electrical stimulation with non-implanted devices for stress urinary incontinence in women.Cochrane Database Syst Rev. 2017 Dec 22;12(12):CD012390. doi: 10.1002/14651858.CD012390.pub2. Cochrane Database Syst Rev. 2017. PMID: 29271482 Free PMC article.
-
Feedback or biofeedback to augment pelvic floor muscle training for urinary incontinence in women.Cochrane Database Syst Rev. 2011 Jul 6;(7):CD009252. doi: 10.1002/14651858.CD009252. Cochrane Database Syst Rev. 2011. Update in: Cochrane Database Syst Rev. 2025 Mar 11;3:CD009252. doi: 10.1002/14651858.CD009252.pub2. PMID: 21735442 Updated.
-
[Pelvic floor muscle training programmes: a systematic review].Acta Med Port. 2011 Mar-Apr;24(2):309-18. Epub 2011 May 20. Acta Med Port. 2011. PMID: 22011604 Portuguese.
Cited by
-
Treatment Outcomes of Extracorporeal Magnetic Innervation for Female Stress Urinary Incontinence.J Med Ultrasound. 2025 May 23;33(2):112-115. doi: 10.4103/jmu.JMU-D-25-00022. eCollection 2025 Apr-Jun. J Med Ultrasound. 2025. PMID: 40521328 Free PMC article. Review.
References
-
- Doumouchtsis SK, de Tayrac R, Lee J, et al. . An International Continence Society (ICS)/ International Urogynecological Association (IUGA) joint report on the terminology for the assessment and management of obstetric pelvic floor disorders. Int Urogynecol J. 2023;34(1):1-42. doi:10.1007/s00192-022-05397-x - DOI - PMC - PubMed
-
- Soave I, Scarani S, Mallozzi M, Nobili F, Marci R, Caserta D. Pelvic floor muscle training for prevention and treatment of urinary incontinence during pregnancy and after childbirth and its effect on urinary system and supportive structures assessed by objective measurement techniques. Arch Gynecol Obstet. 2019;299(3):609-623. doi:10.1007/s00404-018-5036-6 - DOI - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
