

Widespread pain phenotypes impact treatment efficacy results in randomized clinical trials for interstitial cystitis/bladder pain syndrome: a Multidisciplinary Approach to the Study of Chronic Pelvic Pain network study
- PMID: 39499552
- PMCID: PMC12004979
- DOI: 10.1097/j.pain.0000000000003455
Widespread pain phenotypes impact treatment efficacy results in randomized clinical trials for interstitial cystitis/bladder pain syndrome: a Multidisciplinary Approach to the Study of Chronic Pelvic Pain network study
Abstract
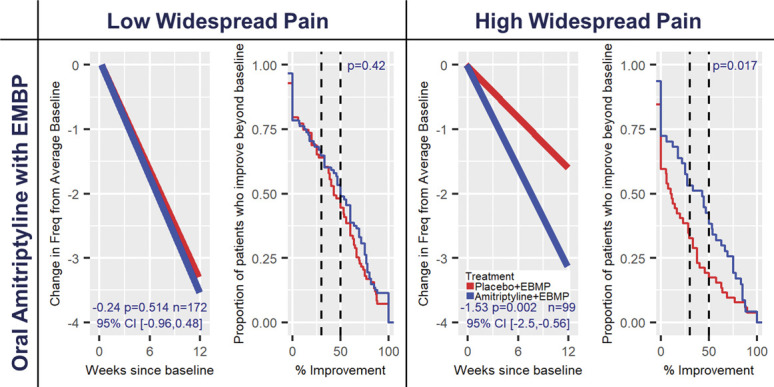
Pain clinical trials are notoriously complex and often inefficient in demonstrating efficacy, even for known efficacious treatments. A major issue is the difficulty in the a priori identification of specific phenotypes to include in the study population. Recent work has identified the extent of widespread pain as an important determinant of the likelihood of response to therapy, but it has not been tested in clinical trials for the treatment of interstitial cystitis/bladder pain syndrome (IC/BPS). We explored this hypothesis using data from 3 previously published trials testing treatments for IC/BPS, which suggested modest benefits but did not meet a priori primary outcome statistical significance criteria. Importantly, these studies also collected symptom questionnaire data that allowed us to retrospectively identify participants with and without widespread pain. Analyzing the treatment by the degree of widespread pain revealed a difference in outcome and statistical significance level for each trial. Participants with predominately local pain (ie, limited widespread pain symptoms) responded to therapy targeting local symptoms, whereas those with widespread pain did not. Alternatively, participants with widespread pain beyond their local pelvic pain responded to more centrally acting treatments. Our results suggest that differentiating patients based on widespread vs more localized pain is a key consideration for designing future clinical trials for conditions with variable pain profiles, such as IC/BPS and potentially other pain-based syndromic disorders.
Keywords: Interstitial cystitis; Pain measurement; Pelvic pain; Reanalysis of clinical trial results; Widespread pain.
Copyright © 2025 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the International Association for the Study of Pain.
Conflict of interest statement
J.T.F reports over the past 3 years, funding from NIH-NCATS—UL1 Grant (Co-I), NIH-National Institute of Diabetes, Digestive, and Kidney Disease—U01 Grants (CoI), from NIH-NINDS—U24 Grant (PI), and 2 FDA-BAA Contracts; and compensation for serving on 2 NIH DSMBs. Has served on advisory boards as a consultant on clinical trial methods from Vertex and EicOsis Pharmaceuticals. K.T.L. reports employment with GlaxoSmithKline Pharmaceuticals, which occurred after completion of this study. M.A.P. reports being a site for a clinical trial with Lipella Pharmaceuticals Inc. D.A.W. reports consultant relationship with Swing Therapeutics, Inc, and Community Health Focus, Inc. The remaining authors have no conflicts of interest to declare.
Figures


Update of
-
Widespread Pain Phenotypes Impact Treatment Efficacy Results in Randomized Clinical Trials for Interstitial Cystitis/Bladder Pain Syndrome: A MAPP Network Study.Res Sq [Preprint]. 2023 Feb 23:rs.3.rs-2441086. doi: 10.21203/rs.3.rs-2441086/v1. Res Sq. 2023. Update in: Pain. 2025 May 1;166(5):1179-1190. doi: 10.1097/j.pain.0000000000003455. PMID: 36865104 Free PMC article. Updated. Preprint.
References
-
- Agresti A. Categorical Data Analysis. 2nd ed. New York: John Wiley & Sons, 2002.
-
- Backonja MM, Attal N, Baron R, Bouhassira D, Drangholt M, Dyck PJ, Edwards RR, Freeman R, Gracely R, Haanpaa MH, Hansson P, Hatem SM, Krumova EK, Jensen TS, Maier C, Mick G, Rice AS, Rolke R, Treede RD, Serra J, Toelle T, Tugnoli V, Walk D, Walalce MS, Ware M, Yarnitsky D, Ziegler D. Value of quantitative sensory testing in neurological and pain disorders: NeuPSIG consensus. PAIN 2013;154:1807–19. - PubMed
-
- Bryson HM, Wilde MI. Amitriptyline: a review of its pharmacological properties and therapeutic use in chronic pain states. Drugs Aging 1996;8:459–76. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
