

Anatomical vs. electrophysiological approach for ablation of premature ventricular contractions originating from the left ventricular summit (ISESHIMA-SUMMIT Study)
- PMID: 39499643
- PMCID: PMC11572719
- DOI: 10.1093/europace/euae278
Anatomical vs. electrophysiological approach for ablation of premature ventricular contractions originating from the left ventricular summit (ISESHIMA-SUMMIT Study)
Abstract
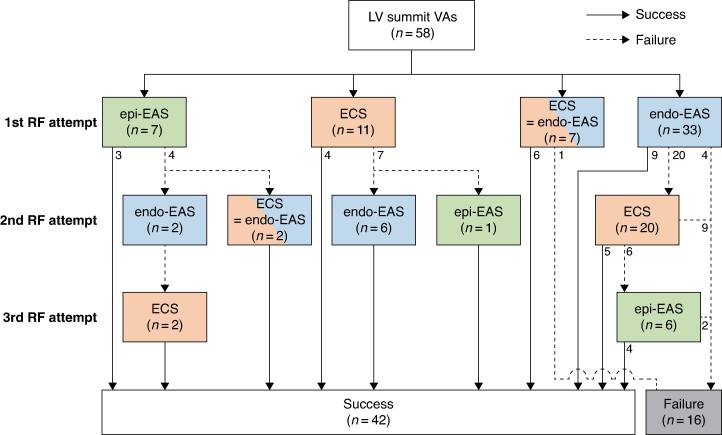
Aims: Catheter ablation (CA) of idiopathic ventricular arrhythmias (VAs) from the epicardial left ventricular summit is challenging. The endocardial approach targets two sites: the endocardial closest site (ECS) to the epicardial earliest activation site (epi-EAS) and the endocardial earliest activation site (endo-EAS). We aimed to differentiate between cases where CA at the ECS was effective and where CA at the endo-EAS yielded success.
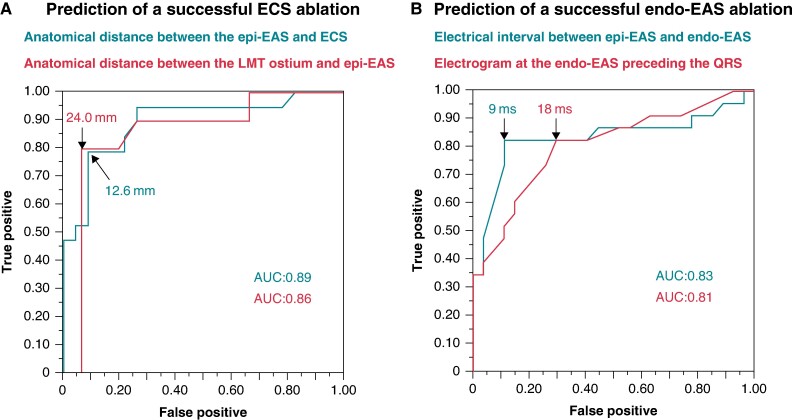
Methods and results: Fifty-eight patients (47 men; age 60 ± 13 years) were analysed with VAs in which the EAS was observed in the coronary venous system (CVS). Overall, VAs were successfully eliminated in 42 (72%) patients: 8 in the CVS, 8 where the ECS matched with the endo-EAS, 11 at the ECS, and 15 at the endo-EAS. A successful ECS ablation was associated with a shorter epi-EAS-ECS distance (10.2 ± 4.7 vs. 18.8 ± 5.3 mm; P < 0.001) and shorter epi-EAS-left main coronary trunk (LMT) ostial distance (20.3 ± 7.6 vs. 30.3 ± 8.4 mm; P = 0.005), with optimal cut-off values of ≤12.6 and ≤24.0 mm, respectively. A successful endo-EAS ablation was associated with an earlier electrogram at the endo-EAS [23 (8, 36) vs. 15 (0, 19) ms preceding the QRS; P < 0.001] and shorter epi-EAS-endo-EAS interval [6 (1, 8) vs. 22 (12, 25) ms; P < 0.001], with optimal cut-off values of ≥18 and ≤9 ms, respectively.
Conclusion: Shorter anatomical distances between the epi-EAS and ECS, and between the epi-EAS and LMT ostium, predict a successful ECS ablation. The prematurity of the endo-EAS electrogram and a shorter interval between the epi-EAS and endo-EAS predicted a successful endo-EAS ablation.
Keywords: Anatomical approach; Electrophysiological approach; Idiopathic ventricular arrhythmias; Left ventricular summit.
© The Author(s) 2024. Published by Oxford University Press on behalf of the European Society of Cardiology.
Conflict of interest statement
Conflict of interest: K.N. received speaker honoraria from Johnson & Johnson, Medtronic Japan, Boston Scientific Japan, Abbott Japan, and Daiichi-Sankyo. S.T. received honoraria from Medtronic Japan, Daiichi-Sankyo, Johnson & Johnson, Boston Scientific Japan, Abbott Japan, Bayer Yakuhin, and Japan Lifeline and is affiliated with the endowed research courses supported by Medtronic Japan, Japan Lifeline, Boston Scientific Japan, Abbott Japan, and Biotronik Japan. Y.O. received research grants unrelated to this study from Johnson & Johnson KK and Biosense Webster, Inc., scholarship funds from Nippon Boehringer Ingelheim, and remuneration from Daiichi-Sankyo, AstraZeneca, Bayer Healthcare, Bristol-Myers Squibb, and Johnson & Johnson KK and additionally belongs to the endowed departments of Boston Scientific Japan, Biotronik Japan, Abbott Medical Japan, Japan Lifeline, and Medtronic Japan. All remaining authors have declared no conflicts of interest.
Figures



References
-
- Nagashima K, Choi EK, Lin KY, Kumar S, Tedrow UB, Koplan BA et al. Ventricular arrhythmias near the distal great cardiac vein: challenging arrhythmia for ablation. Circ Arrhythm Electrophysiol 2014;7:906–12. - PubMed
-
- Hayashi T, Santangeli P, Pathak RK, Muser D, Liang JJ, Castro SA et al. Outcomes of catheter ablation of idiopathic outflow tract ventricular arrhythmias with an R wave pattern break in lead V2: a distinct clinical entity. J Cardiovasc Electrophysiol 2017;28:504–14. - PubMed
-
- Komatsu Y, Nogami A, Shinoda Y, Masuda K, Machino T, Kuroki K et al. Idiopathic ventricular arrhythmias originating from the vicinity of the communicating vein of cardiac venous systems at the left ventricular summit. Circ Arrhythm Electrophysiol 2018;11:e005386. - PubMed
-
- Yamada T, McElderry HT, Doppalapudi H, Okada T, Murakami Y, Yoshida Y et al. Idiopathic ventricular arrhythmias originating from the left ventricular summit: anatomic concepts relevant to ablation. Circ Arrhythm Electrophysiol 2010;3:616–23. - PubMed
-
- Yamada T, Doppalapudi H, Litovsky SH, McElderry HT, Kay GN. Challenging radiofrequency catheter ablation of idiopathic ventricular arrhythmias originating from the left ventricular summit near the left main coronary artery. Circ Arrhythm Electrophysiol 2016;9:e004202. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
