

Ultrasound assessment of the pelvic sidewall: methodological consensus opinion
- PMID: 39499650
- PMCID: PMC11693842
- DOI: 10.1002/uog.29122
Ultrasound assessment of the pelvic sidewall: methodological consensus opinion
Abstract
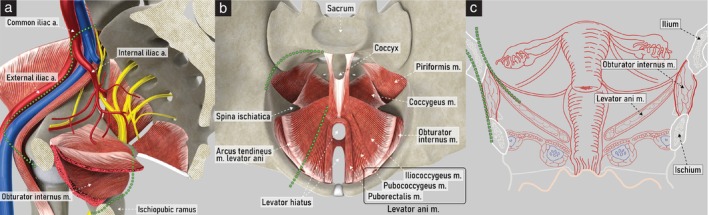
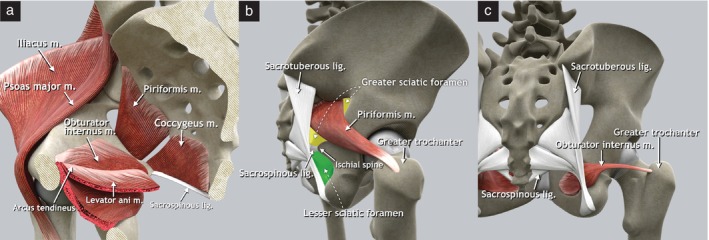
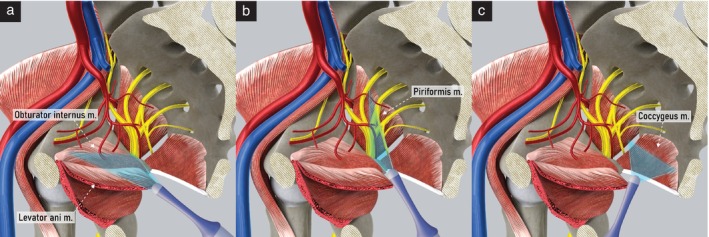
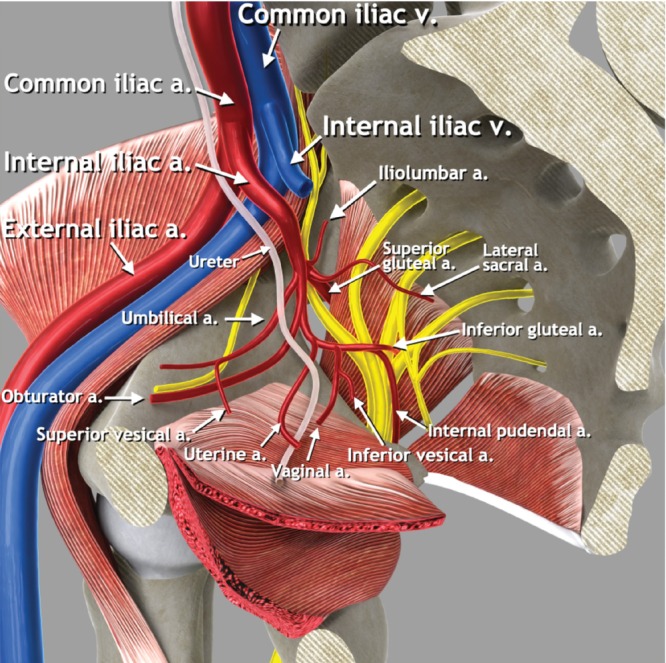
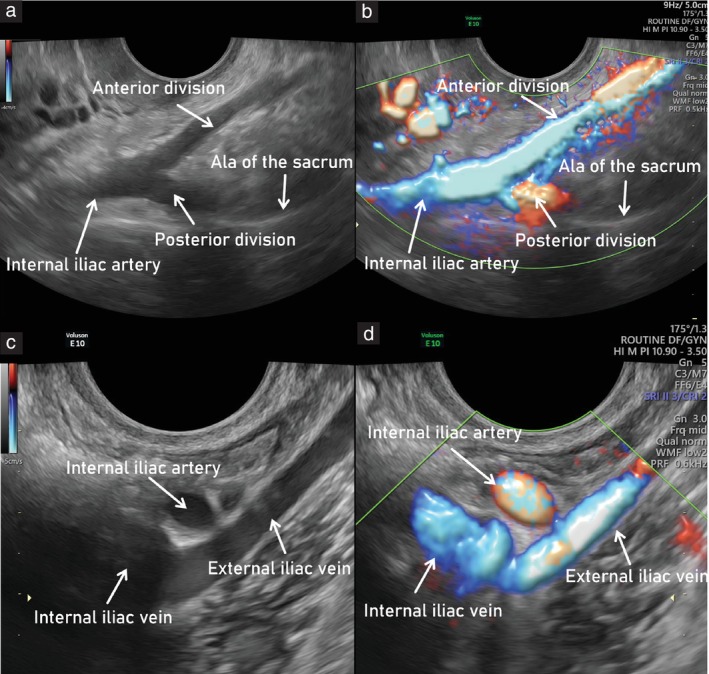
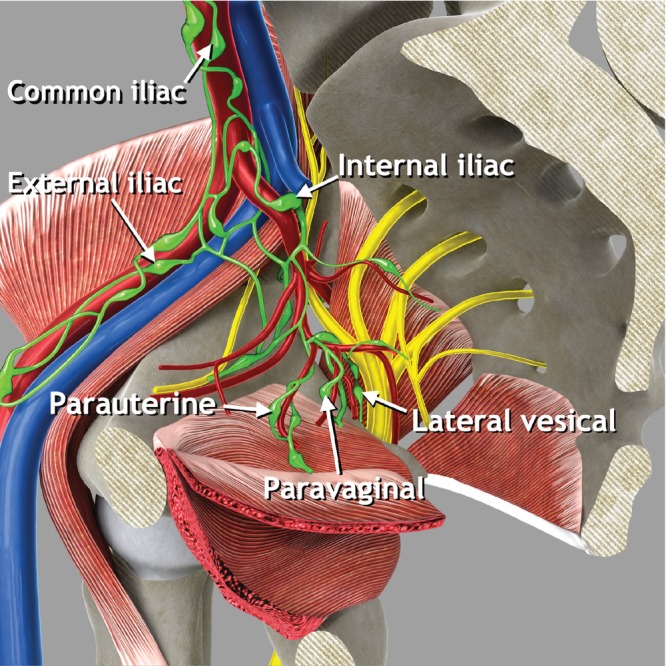
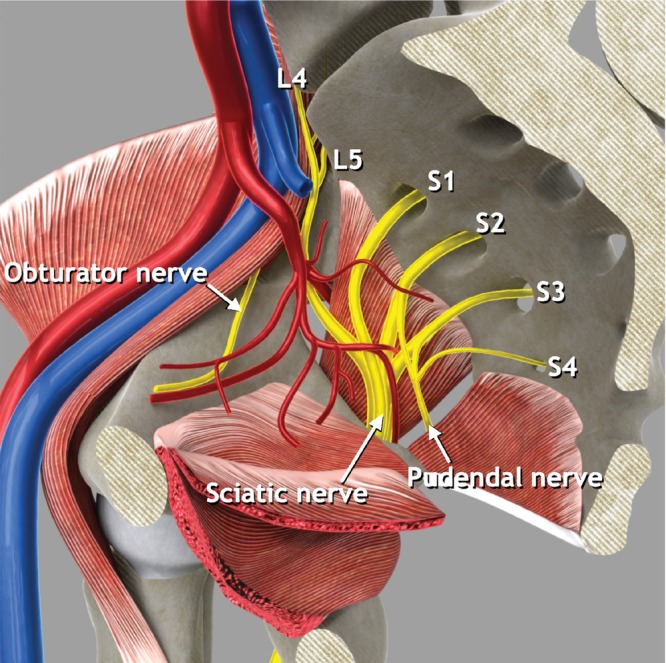
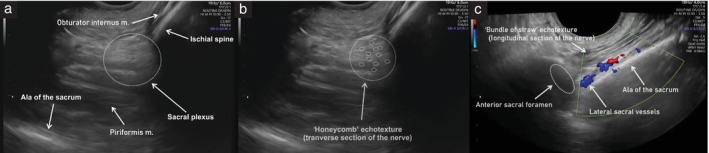
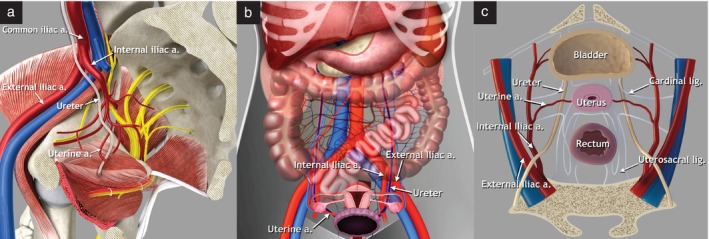
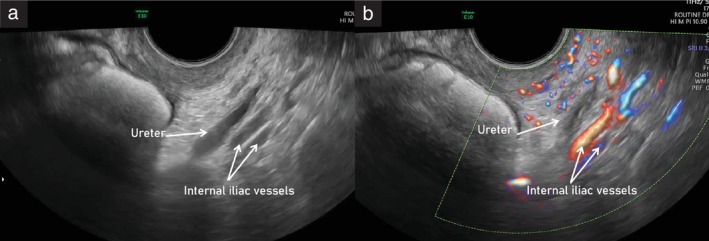
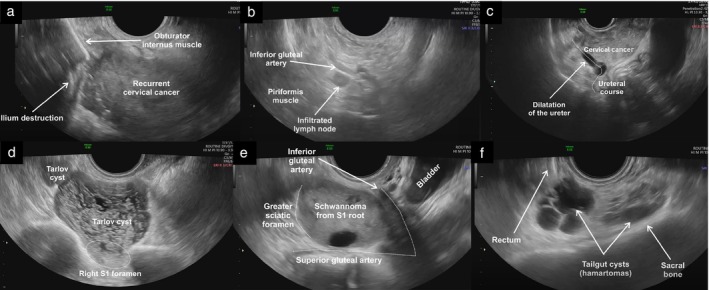
A standardized methodology for the ultrasound evaluation of the pelvic sidewall has not been proposed to date. Herein, a collaborative group of gynecologists and gynecological oncologists with extensive ultrasound experience presents a systematic methodology for the ultrasonographic evaluation of structures within the pelvic sidewall. Five categories of anatomical structures are described (muscles, vessels, lymph nodes, nerves and ureters). A step-by-step transvaginal ultrasound (or, when this is not feasible, transrectal ultrasound) approach is outlined for the evaluation of each anatomical landmark within these categories. Accurate assessment of the pelvic sidewall using a standardized approach improves the detection and diagnosis of non-gynecological pathologies that may mimic gynecological tumors, reducing the risk of unnecessary and even harmful intervention. Furthermore, it plays an important role in completing the staging of malignant gynecological conditions. Transvaginal or transrectal ultrasound therefore represents a viable alternative to magnetic resonance imaging in the preoperative evaluation of lesions affecting the pelvic sidewall, if performed by an expert sonographer. A series of videoclips showing normal and abnormal findings within each respective category illustrates how establishing a universally applicable approach for evaluating this crucial region will be helpful for assessing both benign and malignant conditions affecting the pelvic sidewall. © 2024 The Author(s). Ultrasound in Obstetrics & Gynecology published by John Wiley & Sons Ltd on behalf of International Society of Ultrasound in Obstetrics and Gynecology.
Keywords: anatomy; clinical cases; endometriosis; gynecological tumor; pelvic sidewall; transvaginal ultrasound.
© 2024 The Author(s). Ultrasound in Obstetrics & Gynecology published by John Wiley & Sons Ltd on behalf of International Society of Ultrasound in Obstetrics and Gynecology.
Figures

References
-
- Szabo G, Bokor A, Fancsovits V, et al. Clinical and ultrasound characteristics of deep endometriosis affecting sacral plexus. Ultrasound Obstet Gynecol. 2024;64:104‐111. - PubMed
-
- Guerriero S, Condous G, Rolla M, et al. Addendum to the consensus opinion from the International Deep Endometriosis Analysis (IDEA) group: sonographic evaluation of the parametrium. Ultrasound Obstet Gynecol. 2023;64:275‐280. - PubMed
-
- Timor‐Tritsch IE. Sliding organs sign in gynecological ultrasound. Ultrasound Obstet Gynecol. 2015;46:125‐126. - PubMed
-
- Fischerova D, Santos G, Wong L, et al. Imaging in gynecological disease (26): clinical and ultrasound characteristics of benign retroperitoneal pelvic peripheral‐nerve‐sheath tumors. Ultrasound Obstet Gynecol. 2023;62:727‐738. - PubMed
-
- Ramirez PT, Frumovitz M, Abu‐Rustum NR. Abdominal and pelvic anatomy. Principles of Gynecologic Oncology Surgery. Elsevier; 2021:3‐49.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
