

Preventive Measures and Risk Factors for Post-ERCP Pancreatitis: A Systematic Review and Individual Patient Data Meta-Analysis
- PMID: 39500841
- PMCID: PMC11602798
- DOI: 10.1007/s10620-024-08693-2
Preventive Measures and Risk Factors for Post-ERCP Pancreatitis: A Systematic Review and Individual Patient Data Meta-Analysis
Abstract
Background: Post-endoscopic retrograde cholangiopancreatography (ERCP) pancreatitis (PEP) is the most common complication of ERCP, with limited studies comparing combined prophylactic measures and their efficacy relative to individual patient risk profiles. This study aims to perform an individual patient data meta-analysis (IPDMA) to evaluate the contribution of patient and ERCP-related risk factors to PEP development and to identify the best prophylaxis strategies according to the patient's risk profile.
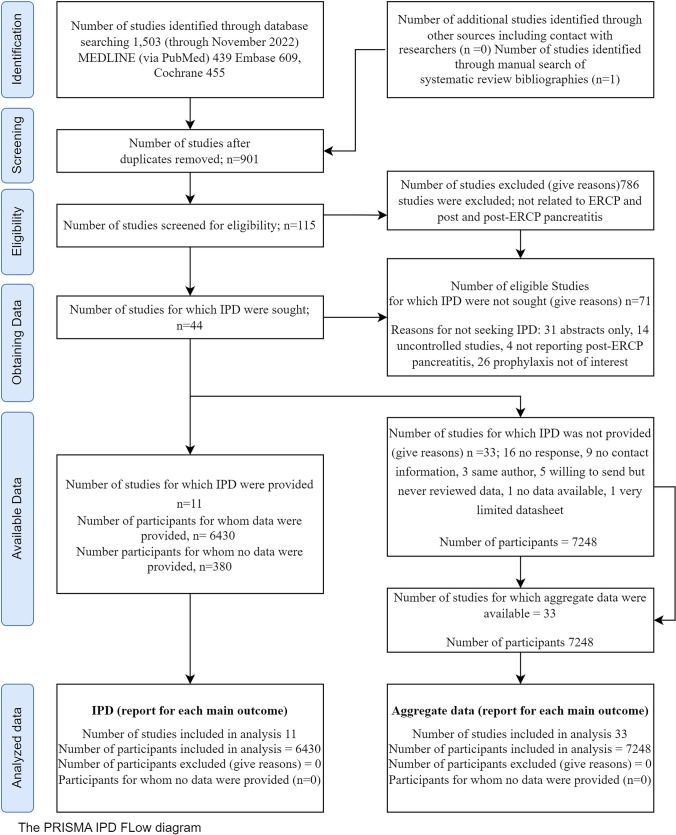
Methods: We systematically searched MEDLINE, Embase, and Cochrane databases until November 2022 for randomized controlled PEP prophylaxis trials. We invited authors to share individual patient data, including PEP risk profile and prophylaxes used. PEP incidence rates for different prophylaxis were calculated. Efficacy was compared using multilevel logistic regression and expressed as relative risk (RR). Subgroup analysis evaluated the role of patient and ERCP-related risk factors in developing PEP.
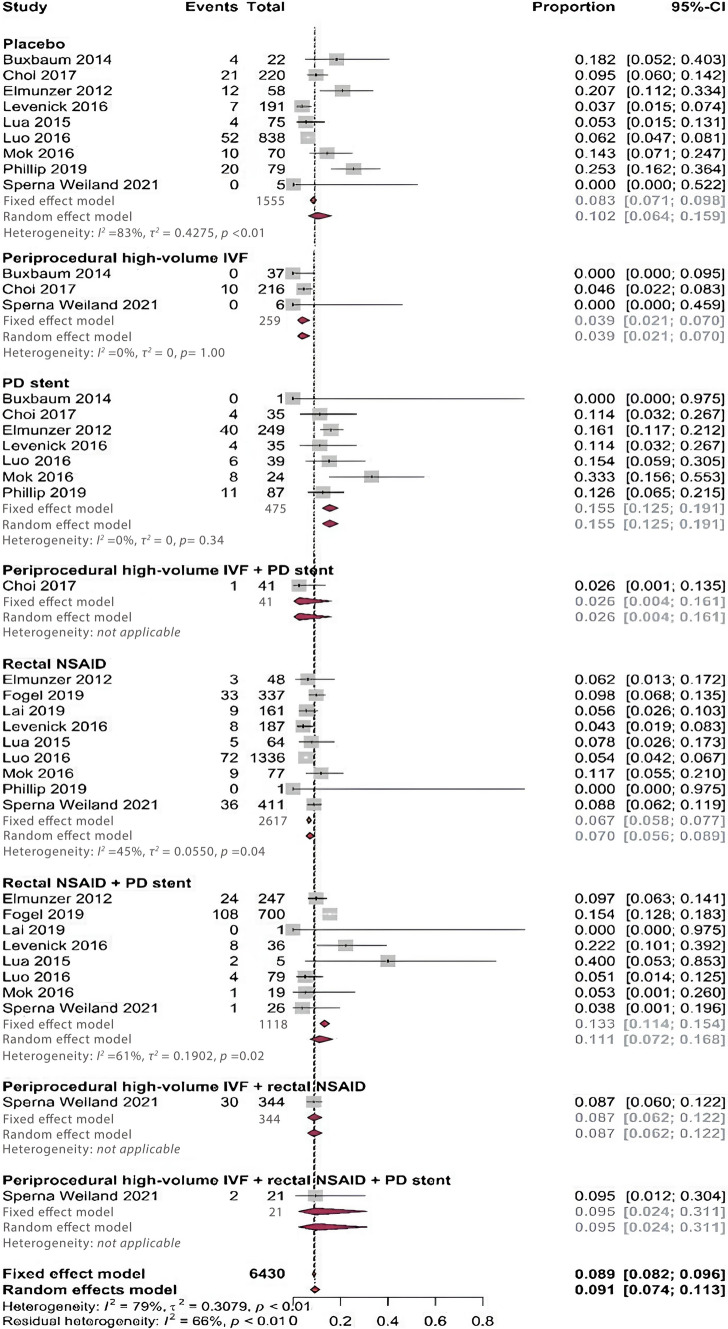
Results: Data from 11 studies, including 6430 patients, were analyzed. After adjusting for risk factors, rectal NSAIDs (RR 0.69, 95%CI 0.54-0.88) and peri-procedural high-volume intravenous fluid (IVF) (RR 0.40, 95%CI 0.21-0.79) were effective in reducing PEP incidence, while no benefit was noted with pancreatic duct (PD) stents (RR 1.25, 95%CI 0.91-1.73). In patients receiving rectal NSAIDs (n = 2617), difficult cannulation (RR 1.99, 1.45-2.73), contrast injection into the pancreatic duct (PD) (RR2.37, 1.68-3.32), and prior history of PEP (RR 1.90, 1.06-3.41) were associated with increased PEP risk.
Conclusion: This IPDMA confirms that rectal NSAIDs and peri-procedural IVF are effective PEP prophylactic strategies. Further studies focusing on combination therapy or the development of personalized PEP risk calculators are needed to improve prophylactic strategies.
Keywords: ERCP; PEP; Pancreatitis; Patient-level meta-analysis; Rectal indomethacin.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Conflict of interest: JPHD has received research funding from Gilead and Abbvie. EJMvG has received research funding from Boston Scientific, Micro-Tech, Pentax, Tae Woong, Olympus, Viatris, and Zambon Medical and served as a consultant for MTW-Endoskopie. PS has received research funding from Pentax, Boston Scientific, Micro-Tech, and The Enose Company. VK reports personal fees from Abbvie, is an advisory board participant for Cook Medical, and receives grants from Orgensis and Theraly. VSA is co-founder and chief medical officer of Origin Endoscopy Inc., Solv Endotherapy Inc. and consultant for Olympus and has received educational grants from Boston Scientific, Medtronic, Abbvie, and Chirhoclin. All other authors declare no competing interests. Ethical approval: N/A. Informed consent: N/A. Registry and the registration no. of study: PROSPERO: registration number CRD42021231197. Animal studies: N/A.
Figures
References
-
- Healthcare Cost and Utilization Project 2020. [cited 2020 May 1]; https://hcupnet.ahrq.gov/
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
