

Genome-first determination of the prevalence and penetrance of eight germline myeloid malignancy predisposition genes: a study of two population-based cohorts
- PMID: 39501104
- PMCID: PMC11794151
- DOI: 10.1038/s41375-024-02436-y
Genome-first determination of the prevalence and penetrance of eight germline myeloid malignancy predisposition genes: a study of two population-based cohorts
Abstract
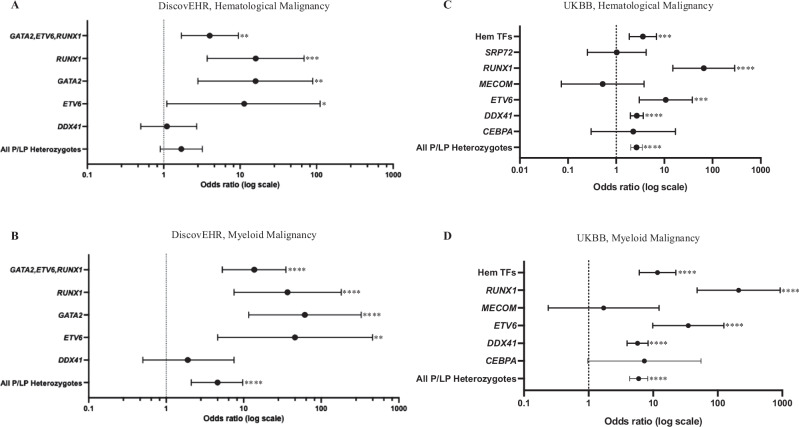
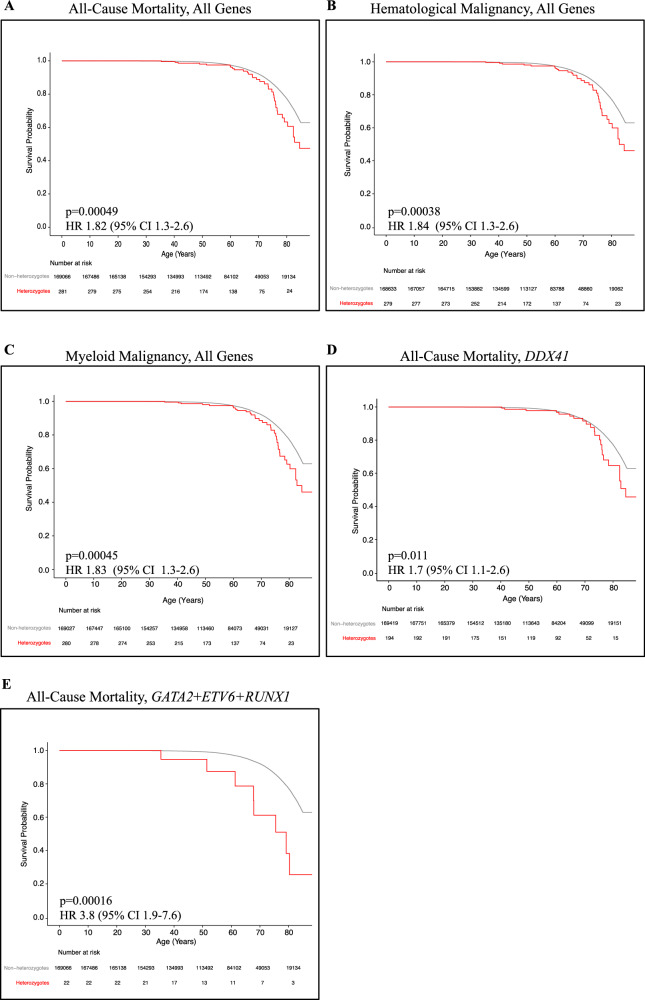
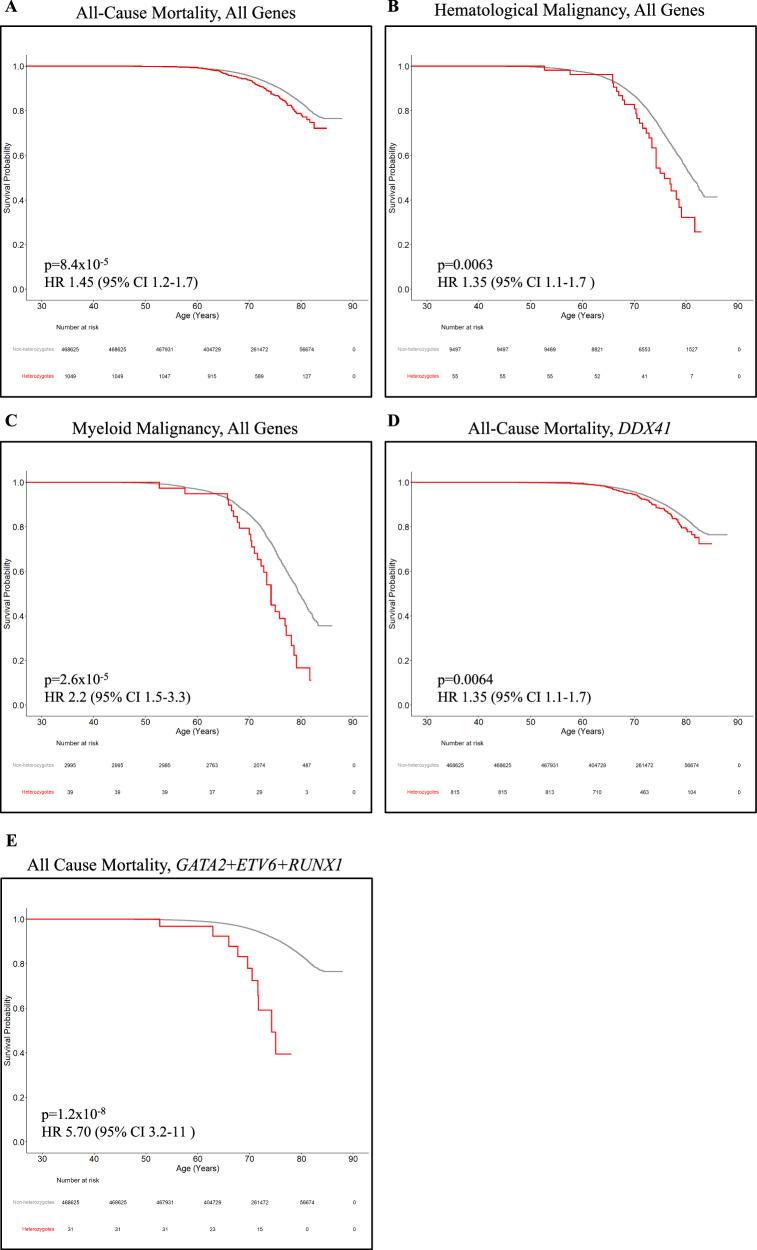
It is estimated that 10% of individuals with a myeloid malignancy carry a germline susceptibility. Using the genome-first approach, in which individuals were ascertained on genotype alone, rather than clinical phenotype, we quantified the prevalence and penetrance of pathogenic germline variants in eight myeloid malignancy predisposition (gMMP) genes. ANKRD26, CEBPA, DDX41, MECOM, SRP72, ETV6, RUNX1 and GATA2, were analyzed from the Geisinger MyCode DiscovEHR (n = 170,503) and the United Kingdom Biobank (UKBB, n = 469,595). We identified a high risk of myeloid malignancies (MM) (odds ratio[OR] all genes: DiscovEHR, 4.6 [95% confidential interval (CI) 2.1-9.7], p < 0.0001; UKBB, 6.0 [95% CI 4.3-8.2], p = 3.1 × 10-27), and decreased overall survival (hazard ratio [HR] DiscovEHR, 1.8 [95% CI 1.3-2.6], p = 0.00049; UKBB, 1.4 [95% CI 1.2-1.8], p = 8.4 × 10-5) amongst heterozygotes. Pathogenic DDX41 variants were the most commonly identified, and in UKBB showed a significantly increased risk of MM (OR 5.7 [95% CI 3.9-8.3], p = 6.0 × 10-20) and increased all-cause mortality (HR 1.35 [95% CI 1.1-1.7], p = 0.0063). Through a genome-first approach, this study genetically ascertained individuals with a gMMP and determined their MM risk and survival.
© 2024. This is a U.S. Government work and not under copyright protection in the US; foreign copyright protection may apply.
Conflict of interest statement
Competing interests: The authors declare no conflict of interest. DJ Carey is the principal investigator or co-investigator and draws partial salary support for three studies funded by Regeneron Pharmaceuticals to Geisinger Clinic. One of these supports the enrollment of patients into the MyCode biobank and exome sequencing; the others are studies of individuals with genetic variants associated with clonal hematopoiesis of indeterminate potential and GAA deficiency (Pompe disease). R Hendricks, J Kim, ML Ramos, DR Stewart and LJ McReynolds’ work has been funded by the Intramural Research Program of the National Cancer Institute. JS Haley, UL Mirshahi and DJ Carey’s work is funded by Geisinger Medical Center.
Figures


References
-
- Tawana K, Brown AL, Churpek JE. Integrating germline variant assessment into routine clinical practice for myelodysplastic syndrome and acute myeloid leukaemia: current strategies and challenges. Br J Haematol. 2022;196:1293–310. - PubMed
-
- Samaraweera SE, Wang PPS, Li KL, Casolari DA, Feng J, Pinese M, et al. Childhood acute myeloid leukemia shows a high level of germline predisposition. Blood 2021;138:2293–8. - PubMed
MeSH terms
Grants and funding
- Intramural Research Program/U.S. Department of Health & Human Services | NIH | NCI | Division of Cancer Epidemiology and Genetics, National Cancer Institute (National Cancer Institute Division of Cancer Epidemiology and Genetics)
- NA/Geisinger Health System Foundation
- NA/Regeneron Pharmaceuticals (Regeneron Pharmaceuticals, Inc.)
LinkOut - more resources
Full Text Sources
