

Polygenic Risk of Epilepsy and Poststroke Epilepsy
- PMID: 39502073
- PMCID: PMC11653790
- DOI: 10.1161/STROKEAHA.124.047459
Polygenic Risk of Epilepsy and Poststroke Epilepsy
Abstract
Background: Epilepsy is highly heritable, with numerous known genetic risk loci. However, the genetic predisposition's role in poststroke epilepsy (PSE) remains understudied. This study assesses whether a higher genetic predisposition to epilepsy raises poststroke survivor's risk of PSE.
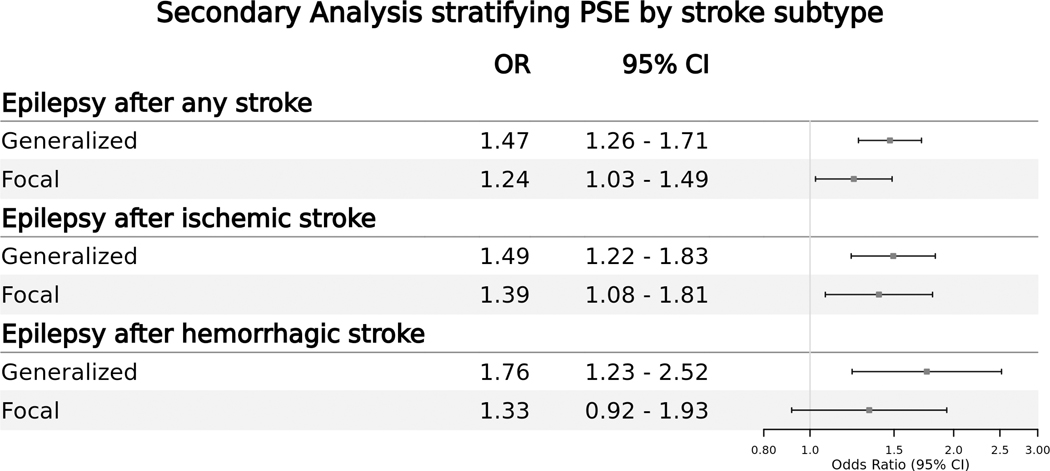
Methods: We conducted a case-control genetic association study nested within the UK Biobank, a large UK-based prospective cohort. Our exposures of interest were 2 distinct polygenic risk scores-generalized and focal epilepsy-modeled as deciles and constructed using genetic variants identified in the latest International League Against Epilepsy genome-wide association study meta-analysis. We aimed to evaluate the association between these polygenic risk scores and their corresponding subtype of PSE-generalized and focal. In sensitivity analyses, we evaluated participants of European ancestry separately and considered focal and generalized epilepsy outcomes in participants without a history of stroke. In secondary analyses, we evaluated the polygenic risk of PSE by stroke subtype (ischemic, hemorrhagic, or any stroke). Multivariable logistic regression models were fitted, adjusting for age, sex, genetic ancestry, and the first 5 principal genetic components.
Results: Among 17 549 UK Biobank stroke survivors with available genetic information (mean age, 61; 43% female), 185 (1%) developed generalized PSE, while 124 (0.7%) developed focal PSE. Multivariable logistic regression results showed that, when compared against the lowest decile, participants within the highest PRS decile for generalized PSE had 5-fold higher odds of developing generalized PSE (OR, 5.05 [95% CI, 2.37-12.5]; P trend<0.001). Similarly, when compared against the lowest decile, participants within the highest polygenic risk score decile for focal PSE had 3-fold higher odds of developing focal PSE (OR, 3.20; [5% CI, 1.25-9.82]; P trend=0.024). Sensitivity analyses among participants of European ancestry yielded similar results.
Conclusions: Our findings suggest that, like other forms of epilepsy, genetic predisposition plays an essential role in PSE. These results underscore the need for future studies to elucidate the mechanisms underlying PSE development and to identify novel therapeutic avenues.
Keywords: epilepsy; genetic risk score; genetics; poststroke epilepsy; stroke.
Conflict of interest statement
All authors declare no financial relationships with any organizations that might have had an interest in the submitted work in the previous 3 years and no other relationships or activities that could seem to have influenced the submitted work. Dr Rivier reports grants from Pyxis partners. Dr de Havenon has received investigator-initiated clinical research funding from the National Institutes of Health, consultant fees from Novo Nordisk, royalty fees from UpToDate, and equity in TitinKM and Certus. Dr Zelano reports speaker honoraria for unbranded educational events from UCB and Eisai, royalties/writer honoraria from Liber AB, Neurologi i Sverige, Studentlitteratur AB, and Wiley; as an employee of Sahlgrenska University Hospital being principal investigator/sub-investigator in clinical trials sponsored by Bial, SK Life science, GW Pharma, and UCB (no personal compensation). Dr Mishra is an editorial board member of the Neurology and convenor of the IPSERC. Dr Mishra is a US Government employee at the Department of Veteran Affairs. To be noted that this article includes NKM’s personal opinions and should not be construed to reflect that of the US Government and the Department of Veteran Affairs. Dr Hirsch reports compensation from Ceribell for consultant services; compensation from Neuropace Inc for other services; compensation from Marinus for consultant services; compensation from Accure for consultant services; compensation from Gilead Sciences Inc for consultant services; compensation from Neurelis Inc for consultant services; compensation from UCB Inc for consultant services; compensation from Natus Medical Incorporated for other services; and compensation from Rapport therapeutics for consultant services. Dr Liebeskind reports compensation from Cerenovus for consultant services; compensation from Stryker for consultant services; compensation from Rapid Medical Ltd for consultant services; compensation from Medtronic for consultant services; and compensation from Genentech for consultant services. Dr Gilmore reports compensation from UCB for consultant services. Dr Mazumder was supported by the Fogarty International Center of the National Institutes of Health under Award Number K01TW012178. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. Dr Sheth reports compensation from Bexorg for consultant services; employment by Yale School of Medicine; compensation from Sense for data and safety monitoring services; compensation from Philips for data and safety monitoring services; compensation from Astrocyte for consultant services; stock holdings in AbbVie; compensation from Cerevasc for consultant services; compensation from Rhaeos for consultant services; stock options in BrainQ; a patent pending for Stroke wearables licensed to Alva Health; and grants from Hyperfine. Dr Worrall reports compensation from American Academy of Neurology for other services.
Figures


Update of
-
Polygenic Risk of Epilepsy and Post-Stroke Epilepsy.medRxiv [Preprint]. 2023 Sep 18:2023.09.18.23295739. doi: 10.1101/2023.09.18.23295739. medRxiv. 2023. Update in: Stroke. 2024 Dec;55(12):2835-2843. doi: 10.1161/STROKEAHA.124.047459. PMID: 37790357 Free PMC article. Updated. Preprint.
Comment in
-
Can Genetics Improve Prediction of Poststroke Epilepsy?Stroke. 2024 Dec;55(12):2844-2845. doi: 10.1161/STROKEAHA.124.049298. Epub 2024 Nov 6. Stroke. 2024. PMID: 39502035 No abstract available.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
