

Comparative Efficacy and Safety of Direct Oral Anticoagulants Versus Warfarin in Atrial Fibrillation Patients with Chronic Liver Disease: A Systematic Review and Meta-analysis
- PMID: 39502439
- PMCID: PMC11534343
- DOI: 10.19102/icrm.2024.15103
Comparative Efficacy and Safety of Direct Oral Anticoagulants Versus Warfarin in Atrial Fibrillation Patients with Chronic Liver Disease: A Systematic Review and Meta-analysis
Abstract
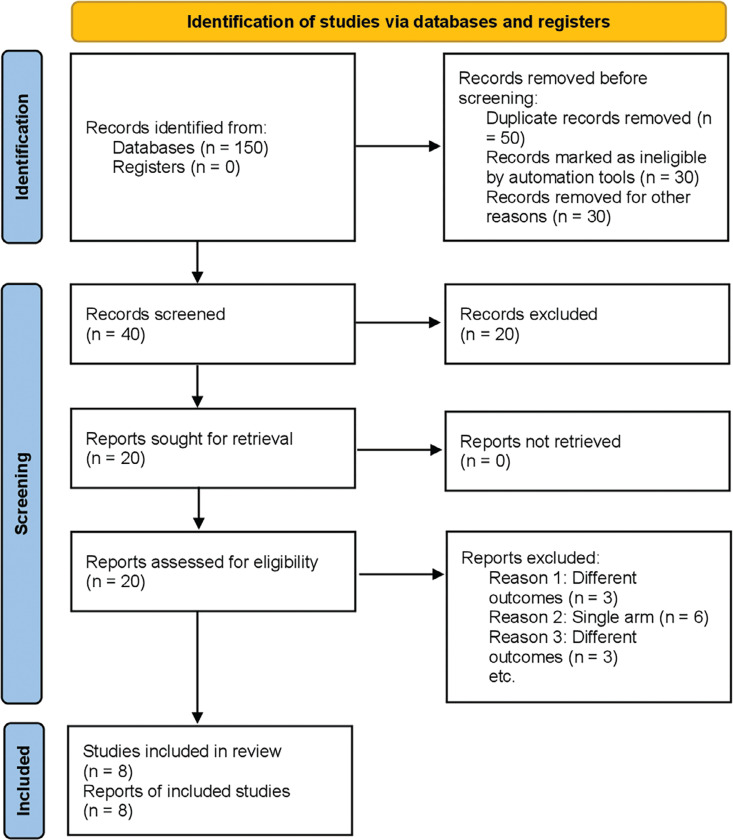
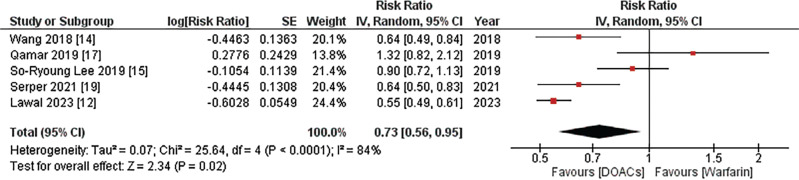
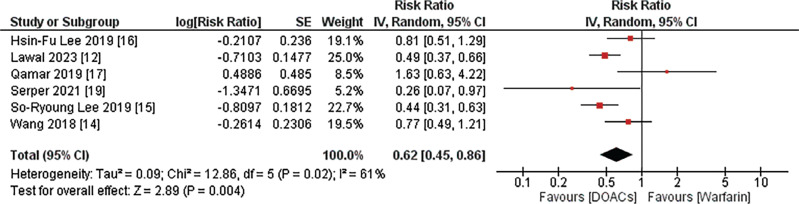
Atrial fibrillation (AF) is a prevalent cardiac arrhythmia. Direct oral anticoagulants (DOACs), with superior efficacy and safety, have emerged as a promising alternative to warfarin. This systematic review and meta-analysis aimed to compare the safety and efficacy of DOACs and warfarin in patients with AF and chronic liver disease (CLD). A systematic search was undertaken in PubMed, the Cochrane Library, and Google Scholar to identify studies comparing the effectiveness of DOACs and warfarin in patients diagnosed with AF and CLD. Subsequent analyses were carried out using the random-effects model. This meta-analysis included eight studies involving 20,684 participants; baseline characteristics indicated a prevalent male presence (56.7%), with an average age of 61.63 ± 9 years. Primary outcomes demonstrated that DOACs were associated with significantly reduced all-cause mortality (relative risk [RR], 0.73; 95% confidence interval [CI], 0.56-0.95; I 2 = 84%; P = .02) and ischemic stroke risk (RR, 0.62; 95% CI, 0.45-0.86; I 2 = 61%; P = .004). Secondary outcomes revealed a significantly reduced risk of major bleeding with DOACs compared to warfarin, while gastrointestinal bleeding showed a non-significant decrease. Intracranial hemorrhage risk was significantly lower with DOACs compared to warfarin. DOACs demonstrate superior safety and efficacy compared to warfarin, evidenced by reduced rates of all-cause death, ischemic stroke, severe bleeding, and cerebral hemorrhage. Further randomized controlled trials are essential to enhance the evidence base for DOACs across diverse patient populations.
Keywords: Atrial fibrillation; DOACs; chronic liver disease; direct oral anticoagulants; meta-analysis; warfarin.
Copyright: © 2024 Innovations in Cardiac Rhythm Management.
Conflict of interest statement
The authors report no conflicts of interest for the published content. No funding information was provided.
Figures
Similar articles
-
Periprocedural Outcomes of Direct Oral Anticoagulants Versus Warfarin in Nonvalvular Atrial Fibrillation.Circulation. 2018 Oct 2;138(14):1402-1411. doi: 10.1161/CIRCULATIONAHA.117.031457. Circulation. 2018. PMID: 29794081
-
Direct Oral Anticoagulants vs. Warfarin in Latin American Patients With Atrial Fibrillation: Evidence From Four post-hoc Analyses of Randomized Clinical Trials.Front Cardiovasc Med. 2022 Mar 4;9:841341. doi: 10.3389/fcvm.2022.841341. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 35310968 Free PMC article.
-
Direct Oral Anticoagulants vs. Vitamin K Antagonists in Atrial Fibrillation Patients at Risk of Falling: A Meta-Analysis.Front Cardiovasc Med. 2022 May 9;9:833329. doi: 10.3389/fcvm.2022.833329. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 35615562 Free PMC article.
-
Comparative Effectiveness and Safety of Direct Oral Anticoagulants and Warfarin in Patients With Atrial Fibrillation and Chronic Liver Disease: A Nationwide Cohort Study.Circulation. 2023 Mar 7;147(10):782-794. doi: 10.1161/CIRCULATIONAHA.122.060687. Epub 2023 Feb 10. Circulation. 2023. PMID: 36762560
-
Effectiveness and Safety of Direct Oral Anticoagulants in an Asian Population with Atrial Fibrillation Undergoing Dialysis: A Population-Based Cohort Study and Meta-Analysis.Cardiovasc Drugs Ther. 2021 Oct;35(5):975-986. doi: 10.1007/s10557-020-07108-4. Epub 2020 Nov 19. Cardiovasc Drugs Ther. 2021. PMID: 33211254
References
-
- Proietti M, Marzona I, Vannini T, et al. Impact of liver disease on oral anticoagulant prescription and major adverse events in patients with atrial fibrillation: analysis from a population-based cohort study. Eur Heart J Cardiovasc Pharmacother. 2021;7(FI1):f84–f92. doi: 10.1093/ehjcvp/pvaa015. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources