

Outcomes of Radiofrequency Ablation for Autonomously Functioning Thyroid Adenomas-Mayo Clinic Experience
- PMID: 39502476
- PMCID: PMC11535713
- DOI: 10.1210/jendso/bvae175
Outcomes of Radiofrequency Ablation for Autonomously Functioning Thyroid Adenomas-Mayo Clinic Experience
Abstract
Background: Autonomously functioning thyroid nodules (AFTNs) constitute 5% to 7% of thyroid nodules and represent the second most common cause of hyperthyroidism following Graves' disease. Currently, radioactive iodine (RAI) and surgery are the standard treatment options, and both incur a risk of postprocedural hypothyroidism and other surgery and radiation-related complications.
Methods: This work aimed at assessing the efficacy of radiofrequency ablation (RFA) as an alternative treatment option for resolving hyperthyroidism and the nodule volume rate reduction (VRR) and its associated adverse events.
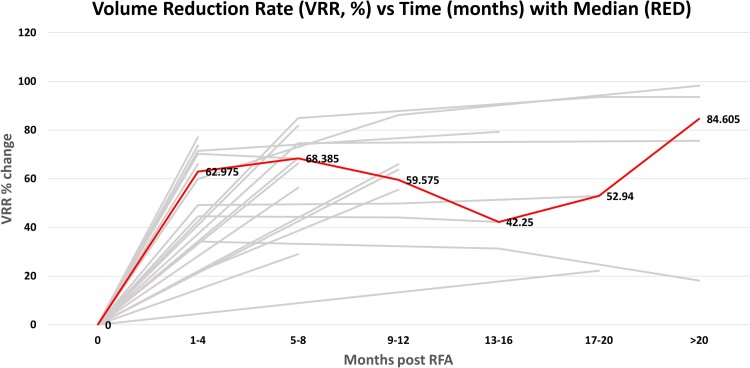
Results: A total of 22 patients underwent RFA for a solitary AFTN. Seventy-two percent (n = 16) had subclinical hyperthyroidism, 9% (n = 2) had overt hyperthyroidism, and 18% (n = 4) were biochemically euthyroid on antithyroid medication. Average pretreatment TSH was 0.41 mIU/L (SD = 0.98) and free T4 1.29 ng/dL (SD = 0.33). Following a single RFA session, hyperthyroidism resolved in 90.9% (n = 20) and average VRR (61.13%) was achieved within 3 to 6 months following the ablation. Except for 1 nodule, none of the nodules grew during the follow-up period (16.5 months). Two patients (9%) developed transient tachycardia requiring short-term beta-blocker therapy, and 2 developed mild hypothyroidism requiring levothyroxine therapy. Two patients developed recurrent hyperthyroidism and elected to undergo lobectomy and repeat RFA respectively. No serious adverse effects were noted in this cohort.
Conclusion: RAI and/or surgery represent the standard of care for toxic adenomas, but RFA shows excellent efficacy and safety profile. Therefore, at centers with RFA expertise, it should be considered an alternative treatment strategy, avoiding radiation and surgery-related complications.
Keywords: ablation; autonomous; hyperthyroidism; radioactive iodine; radiofrequency; thyroid nodule.
© The Author(s) 2024. Published by Oxford University Press on behalf of the Endocrine Society.
Figures


References
-
- Magister MJ, Chaikhoutdinov I, Schaefer E, Williams N, Saunders B, Goldenberg D. Association of thyroid nodule size and Bethesda class with rate of malignant disease. JAMA Otolaryngol Head Neck Surg. 2015;141(12):1089‐1095. - PubMed
-
- Kim C, Lee JH, Choi YJ, Kim WB, Sung TY, Baek JH. Complications encountered in ultrasonography-guided radiofrequency ablation of benign thyroid nodules and recurrent thyroid cancers. Eur Radiol. 2017;27(8):3128‐3137. - PubMed
-
- Hodax JK, Reinert SE, Quintos JB. Autonomously functioning thyroid nodules in patients <21 years of age: the Rhode Island hospital experience from 2003-2013. Endocr Pract. 2016;22(3):328‐337. - PubMed
-
- Niedziela M, Breborowicz D, Trejster E, Korman E. Hot nodules in children and adolescents in western Poland from 1996 to 2000: clinical analysis of 31 patients. J Pediatr Endocrinol Metab. 2002;15(6):823‐830. - PubMed
LinkOut - more resources
Full Text Sources