

The impact of door to extracorporeal cardiopulmonary resuscitation time on mortality and neurological outcomes among out-of-hospital cardiac arrest acute myocardial infarction patients treated by primary percutaneous coronary intervention
- PMID: 39503005
- PMCID: PMC11535889
- DOI: 10.1016/j.ahjo.2024.100473
The impact of door to extracorporeal cardiopulmonary resuscitation time on mortality and neurological outcomes among out-of-hospital cardiac arrest acute myocardial infarction patients treated by primary percutaneous coronary intervention
Abstract
Background: Few previous studies evaluated the impact of time from the hospital arrival to the implementation of extracorporeal cardiopulmonary resuscitation (ECPR) (door to ECPR time) on outcomes among out-of-hospital cardiac arrest (OHCA) acute myocardial infarction (MI) patients.
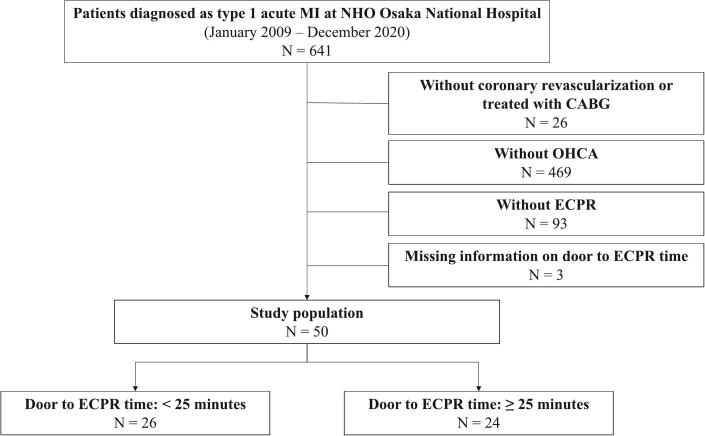
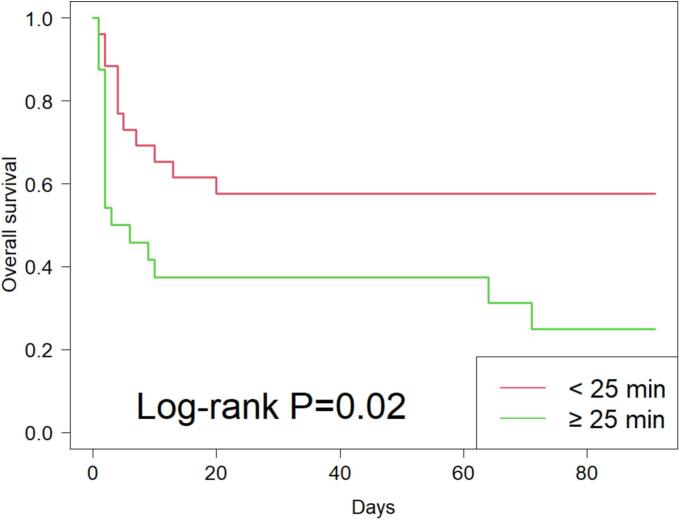
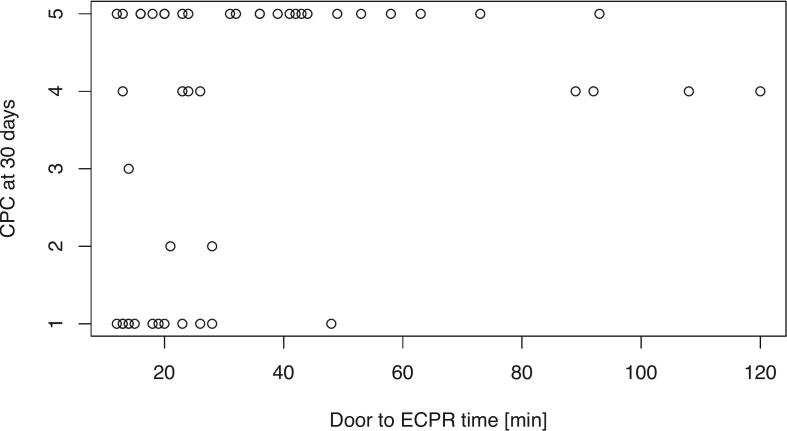
Methods: 50 patients with OHCA who received both ECPR and percutaneous coronary intervention (PCI) at Cardiovascular Division, NHO Osaka National Hospital were analyzed. Patients were divided into 2 groups according to the median of door to ECPR time. The primary outcome was all-cause death. Survival analyses were conducted to compare all-cause mortality at 90 days between 2 groups. Neurological outcome at 30 days was also compared between 2 groups using the Cerebral Performance Category (CPC).
Results: The multivariable Cox proportional-hazards model showed that all-cause mortality at 90 days was significantly higher among patients with door to ECPR time ≥ 25 min compared with those with door to ECPR time < 25 min (adjusted hazard ratio [HR]: 3.14; 95 % confidence interval [CI]: 1.21-8.18). The proportion of patients with CPC at 30 days ≤ 2 was significantly higher among patients with shorter door to ECPR time (P = 0.048).
Conclusion: Among patients with OHCA due to acute MI who received ECPR and PCI, the shorter door to ECPR time was associated with the lower mortality and favorable neurological outcomes.
Keywords: Extracorporeal cardiopulmonary resuscitation; Myocardial infarction; Out-of-hospital cardiac arrest; Percutaneous coronary intervention.
© 2024 The Authors.
Conflict of interest statement
The authors declare the following financial interests/personal relationships which may be considered as potential competing interests: Yasunori Ueda reports a relationship with 10.13039/100001316Abbott, 10.13039/501100002973Daiichi-Sankyo, Teijin, Japan Lifeline, OrbusNeich, Janssen, Otsuka, Ono, Eli Lilly, Astellas, 10.13039/100002429Amgen, 10.13039/100001003Boehringer Ingelheim, and 10.13039/100004336Novartis that includes: funding grants. Yasunori Ueda reports a relationship with Abbott, Kowa, Bayer, Daiichi-Sankyo, Nipro, Takeda, AstraZeneca, Japan Lifeline, Novartis, Ono, Boehringer Ingelheim, and Amgen that includes: speaking and lecture fees. If there are other authors, they declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
Similar articles
-
The association between time to extracorporeal cardiopulmonary resuscitation and outcome in patients with out-of-hospital cardiac arrest.Eur Heart J Acute Cardiovasc Care. 2022 Jun 7;11(4):279-289. doi: 10.1093/ehjacc/zuac010. Eur Heart J Acute Cardiovasc Care. 2022. PMID: 35143634
-
Neurological outcomes and duration from cardiac arrest to the initiation of extracorporeal membrane oxygenation in patients with out-of-hospital cardiac arrest: a retrospective study.Scand J Trauma Resusc Emerg Med. 2017 Sep 16;25(1):95. doi: 10.1186/s13049-017-0440-7. Scand J Trauma Resusc Emerg Med. 2017. PMID: 28915913 Free PMC article.
-
Revascularization During Cardiac Arrest While Receiving Extracorporeal Life Support in Patients With Acute Myocardial Infarction.JACC Adv. 2024 Dec 13;4(1):101455. doi: 10.1016/j.jacadv.2024.101455. eCollection 2025 Jan. JACC Adv. 2024. PMID: 39759432 Free PMC article.
-
Extracorporeal cardiopulmonary resuscitation versus conventional cardiopulmonary resuscitation in adults with cardiac arrest: a comparative meta-analysis and trial sequential analysis.Lancet Respir Med. 2023 Oct;11(10):883-893. doi: 10.1016/S2213-2600(23)00137-6. Epub 2023 May 22. Lancet Respir Med. 2023. PMID: 37230097
-
Impact of prehospital extracorporeal cardiopulmonary resuscitation for out-of-hospital cardiac arrest on survival with good neurological function: a systematic review and meta-analysis.Resusc Plus. 2025 May 8;24:100974. doi: 10.1016/j.resplu.2025.100974. eCollection 2025 Jul. Resusc Plus. 2025. PMID: 40491772 Free PMC article. Review.
References
-
- Mandigers L., Boersma E., den Uil C.A., Gommers D., Bělohlávek J., Belliato M., Lorusso R., Dos Reis Miranda D. Systematic review and meta-analysis comparing low-flow duration of extracorporeal and conventional cardiopulmonary resuscitation. Interact. Cardiovasc. Thorac. Surg. 2022;35(4) - PMC - PubMed
-
- Matsuyama T., Irisawa T., Yamada T., Hayakawa K., Yoshiya K., Noguchi K., Nishimura T., Ishibe T., Yagi Y., Kiguchi T., Kishimoto M., Shintani H., Hayashi Y., Sogabe T., Morooka T., Sakamoto H., Suzuki K., Nakamura F., Nishioka N., Okada Y., Matsui S., Sado J., Shimazu T., Ohta B., Iwami T., Kitamura T., CRITICAL Study Group Investigators Impact of low-flow duration on favorable neurological outcomes of extracorporeal cardiopulmonary resuscitation after out-of-hospital cardiac arrest: a multicenter prospective study. Circulation. 2020;141(12):1031–1033. - PubMed
-
- Maekawa K., Tanno K., Hase M., Mori K., Asai Y. Extracorporeal cardiopulmonary resuscitation for patients with out-of-hospital cardiac arrest of cardiac origin: a propensity-matched study and predictor analysis. Crit. Care Med. 2013;41(5):1186–1196. - PubMed
-
- Blumenstein J., Leick J., Liebetrau C., Kempfert J., Gaede L., Groß S., Krug M., Berkowitsch A., Nef H., Rolf A., Arlt M., Walther T., Hamm C.W., Möllmann H. Extracorporeal life support in cardiovascular patients with observed refractory in-hospital cardiac arrest is associated with favourable short and long-term outcomes: a propensity-matched analysis. Eur. Heart J. Acute Cardiovasc. Care. 2016;5(7):13–22. - PubMed
-
- Kim S.J., Kim H.J., Lee H.Y., Ahn H.S., Lee S.W. Comparing extracorporeal cardiopulmonary resuscitation with conventional cardiopulmonary resuscitation: a meta-analysis. Resuscitation. 2016;103:106–116. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
